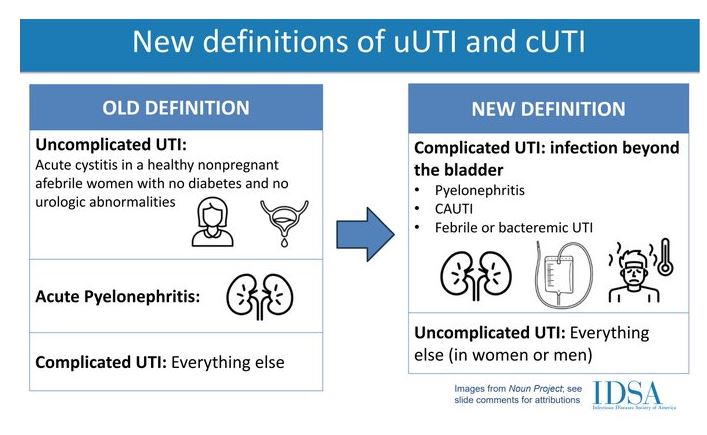
Please note that the current UTI guidelines don’t really meet practice. IDSA is due with new guidelines and a preview was presented at ID week in 2023/ECCMID 2024. It will change the definition of complicated UTIs to include pyelonephritis, catheter-associated UTI (CAUTI), UTI with fever or other evidence of systemic or upper tract infection and uncomplicated UTI to be everything else. Classically guidelines suggest all UTI in men are complicated, but that’s not the case (must look for prosthetic involvement). See slides at the end.
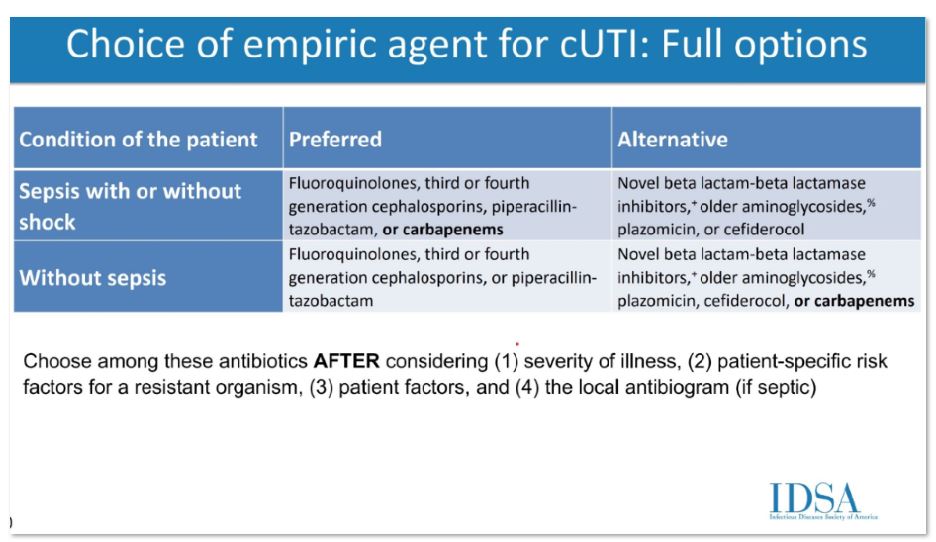
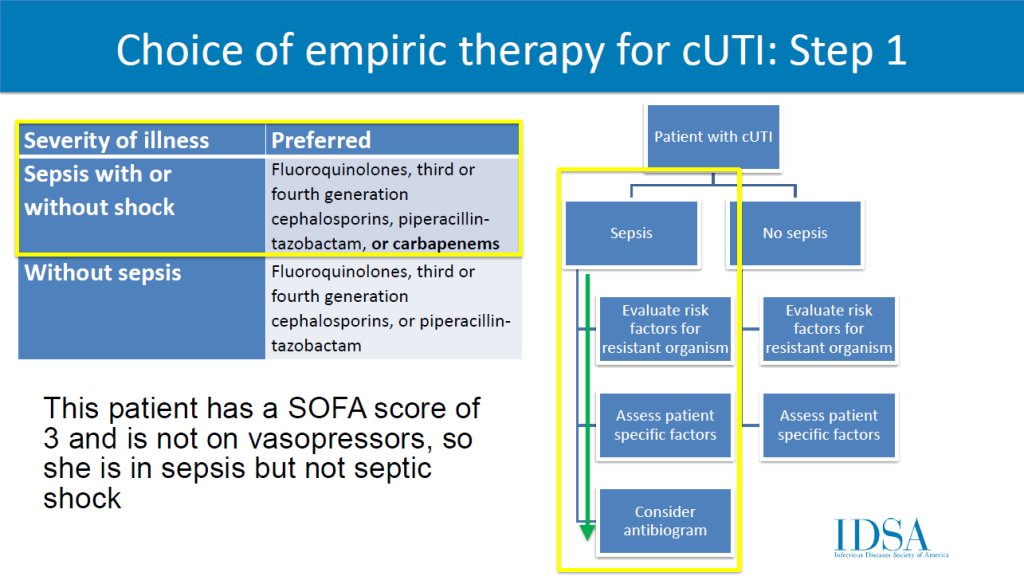
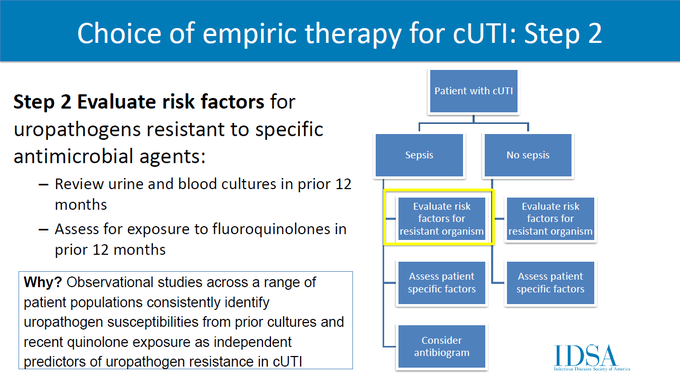
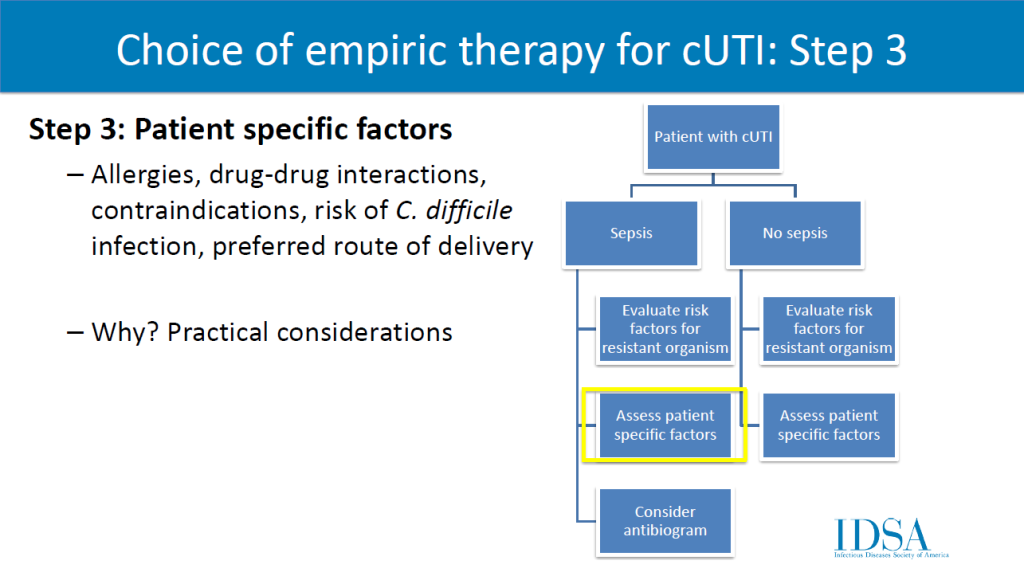
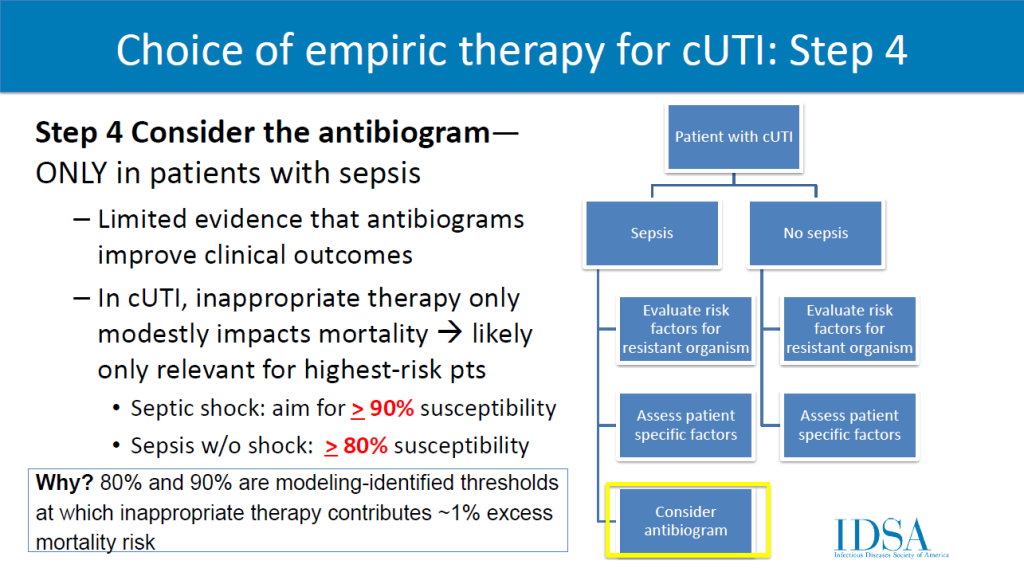
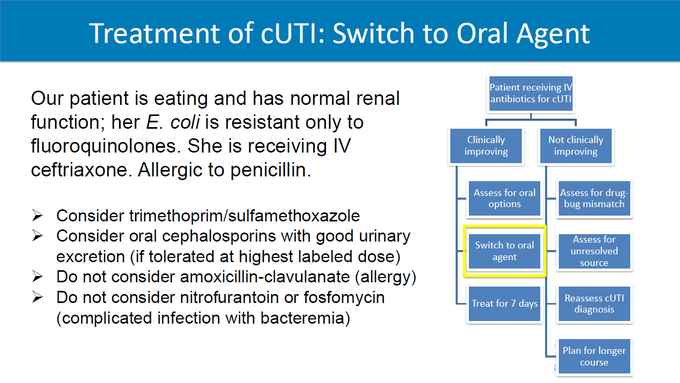
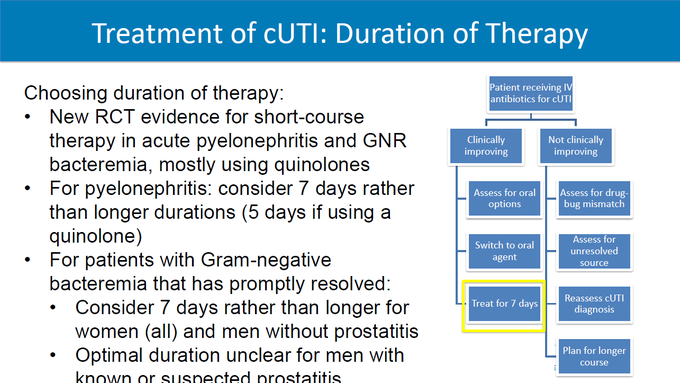
The selection of empiric antibiotics for complicated UTI will include a four-step process. Clinicians should review (1) severity of illness, (2) risk factors for resistant organisms, (3) patient factors, and (4, only if septic) antibiogram. Preferred agents: fluoroquinolones, 3rd/4th generation cephalosporins, piperacillin-tazobactam, (if septic) carbapenems. A 7 day duration is recommended rather than a longer course if clinical improvement is demonstrated.
WikiGuidelines recently (11/2024) introduced guidelines that are similar to the proposed IDSA ones.
These are CURRENT guidelines, but may not be current practice:
- 2009 IDSA Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adult
- 2010 IDSA/ESMID International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women
- 2019 IDSA Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria
- 2022 AUA/CUA/SUFU Recurrent Uncomplicated Urinary Tract Infections in Women
- 2024 WikiGuidelines: Guidelines for the Prevention, Diagnosis, and Management of Urinary Tract Infections in Pediatrics and Adults
When presented with a urinary tract infection, you have to ask:
- Cystitis or pyelonephritis?
- Lower UTI – cystitis: dysuria, frequent urination, urgency, suprapubic pain, hematuria
- Upper UTI – pyelonephritis: same as above plus systemic symptoms like fever chills, flank pain, CVA tenderness, nausea and vomiting
- Complicated or Uncomplicated
- Complicated: associated with a structural or functional abnormality of the urinary tract or significant medical or surgical comorbidities: indwelling foley catheter, ureteral stents, prostatic hyperplasia, nephrolithiasis, tumor, fibrosis, urethral stricture, voiding disorders like neurogenic bladder or intrinsic renal disease,
- Also consider if patient has recent hospitalization, pregnancy, history of childhood UTI, recent antimicrobial use, immunosuppression
- Recurrent cystitis: an infection within 14 days of the previous antibiotic discontinuation
- Most frequent causes of UTI include: E. coli, K. pneumoniae, S. saprophyticus, Enterococcus spp, Group B Strep, Proteus mirabilis, Pseudomonas, S. aureus, Candida
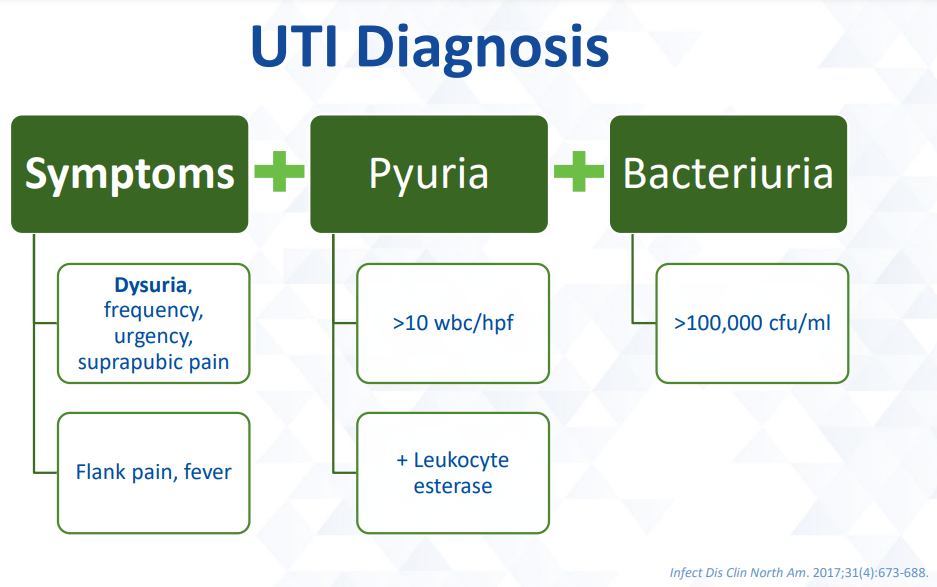
Diagnosis:
Not diagnostic symptoms:
- Altered mental status (AMS)
- Falls
- Malodorous or cloudy urine
- Urinalysis (UA) alone
- Bacteriuria alone
- Leukocyte esterase, nitrites or urine wbc do not
diagnose UTI
Pyuria (“pus” in urine) and bacteriuria (bacteria in urine) are common findings in patients:
% of patients with pyuria:
Young women – 32%
Pregnant women – 30-70%
Women with diabetes – 70%
Elderly institutionalized patients- 90%
Dialysis patients – 90%
Short-term catheters – 30-75%
Long-term catheters – 50-100%
Percent of people with bacteriuria:
Premenopausal women 1-5%
Women 70-90 years old 11-16%
Long-term care residents 15-50%
Females with diabetes 9-29%
Males with diabetes 1-11%
Dialysis patients 25%
Chronic indwelling catheters >90%
These are not diagnostic without symptoms.
(Am J Infect Control. 2017;45(10):1143-1153.)
Treatment:
Asymptomatic Bacteriuria:
DO NOT TREAT ASYMPTOMATIC BACTERIURIA unless your patient is a pregnant women or patient undergoing urologic procedures. All pregnant women should be treated for a positive urine bacteria screen regardless of symptoms. Treatment decreases the risk of pyelonephritis, preterm labor, and low birth weight.
Screening only recommended for asymptomatic people if pregnant or undergoing Transurethral resection of the prostate (TURP) or bladder, ureteroscopy, including lithotripsy, percutaneous nephrolithotomy/nephrolithotripsy.
Treatment of ASB increases the risk for subsequent symptomatic UTI. (Clin Infect Dis. 2019;68(10):e83-e110. JAMA Intern Med. 2017;177(9):1308–1315. Neurosurgery. 2019;85(5):664-671. Clin Infect Dis. 2012;55(6):771-777). Treating asymptomatic bacteriuria is believed to be a driver of resistance in Enterobacterales. Previous ceftriaxone exposure is one of the predictors of ESBL.
Uncomplicated UTI:
Treat based on microbiology when possible. Although cystitis in males is generally classified in the literature as a complicated urinary tract infection (UTI), it is reasonable to consider a healthy man without a neurogenic bladder who has mild to moderate dysuria, urinary frequency and/or urgency, with no symptoms or signs of infection outside the bladder, as having simple cystitis. They can use the same first line treatment as females.
If inpatient, IV antibiotics are preferred initially, but may transition within 72 hours if improvement. Outpatients usually can be managed orally.
- Uncomplicated cystitis (1, 3, 5 – females, 1, 5, 7 days in males) (no concern that the infection has extended beyond the bladder):
- Fosfomycin (only PO in the US) (1 day):
- Females: 3 g for 1 dose
- Males: 3 g for 1 dose – not a lot of data, but treating lower UTI/prostatitis does have some evidence. This is not preferred.
- Can be used with MDR risk factors
- Bactrim (only if local resistance <20%) (3 days)
- Bactrim DS 160/800 mg PO BID for 3 days in female or 7 days in male (avoid if used for UTI in the last 3 months)
- Nitrofurantoin: ONLY FOR CYSTITIS doesn’t work systemically, only for CrCl >20-30 (5 days)
- Females: 100 mg BID * 5 days
- Males: will not work if prostate involvement (age >35 beware), give for 7 days
- Can be used with MDR risk factors
- Pivmecillinam (new in USA)
- The USA FDA approved dose is 185 mg pivmecillinam orally three times daily for three to seven days (185 mg pivmecillinam base is equivalent to 200 mg of pivmecillinam HCl). In some European countries, the recommended dose is twice that for three to five days.
- Can be used with MDR risk factors
- Second line:
- Fluoroquinolone like Cipro or Levaquin for 3 days (female) or 5 days (male) if persistent. Avoid if other options.
- Beta-lactam for 5-7 days. ( amoxicillin-clavulanate (500 mg twice daily), cefpodoxime (100 mg twice daily), and cefadroxil (500 mg twice daily), each given for five to seven days.
- Shorter courses of beta-lactams have been shown to be inferior
- Fosfomycin (only PO in the US) (1 day):
- Uncomplicated pyelonephritis:
- outpatient:
- Ciprofloxacin 500 mg orally twice daily for 7 days or levofloxacin 750 mg orally daily for 5 days if resistance rates are <10%
- When uropathogen resistance is greater than 10%, consider an initial IV dose of ceftriaxone or an aminoglycoside
- Bactrim orally twice daily for 14 days
- Oral ß-lactam antibiotics after a single dose of IV ß-lactam or aminoglycoside for 10-14 days
- Ciprofloxacin 500 mg orally twice daily for 7 days or levofloxacin 750 mg orally daily for 5 days if resistance rates are <10%
- IV Beta-lactam is preferred initially if patient presents with systemic symptoms and hospitalization is required
- outpatient:
Single Dose Aminoglycosides for UTI
Single doses for UTIs are becoming more popular and supported by the literature. Single-dose aminoglycosides should NOT be recommended as first-line therapy or used for complicated urinary tract infections. They can be considered in patients with acute cystitis with normal renal function and multiple barriers to the standard of care.
- Aminoglycosides have excellent activity against most uropathogens, including drug-resistant Enterobacteriaceae.
- They are eliminated as active drug almost exclusively by the kidneys with concentrations 100-fold greater in the urine than plasma, so aminoglycosides can be used as monotherapy here when they cannot in most other instances.
- The post-antibiotic effect of aminoglycosides may persist for up to 72 hours, so you have long activity.
- Toxicities may be limited with one-time administration.
- The single dose prevents medication access & adherence concerns.
- Aminoglycosides can be administered either the IV or IM route, and therefore, does not necessarily require IV access. Gentamicin may be considered the preferred aminoglycoside based on frequency of use in studies.
- Gentamcin: 5 mg/kg IV/IM once
- Amikacin 15mg/kg IV/IM once
- Tobramycin 5mg/kg IV/IM once
- Underweight [TBW<IBW]: use TBW, Nonobese [TBW 1x to 1.25x IBW]: use IBW or TBW, Obese [TBW >1.25x IBW]: use adjusted body weight
- Goodlet KJ, Benhalima FZ, Nailor MD. A Systematic Review of Single-Dose Aminoglycoside Therapy for Urinary Tract Infection: Is It Time To Resurrect an Old Strategy? Antimicrob Agents Chemother. 2018 Dec 21;63(1):e02165-18. doi: 10.1128/AAC.02165-18. PMID: 30397061; PMCID: PMC6325212.
Complicated UTI:
For complicated UTIs associated with urinary instrumentation or obstruction, remove if possible.
- Complicated UTI
- Source control is the best treatment: Relieve obstruction, exchange catheters, drain infected fluid collections
- Intravenous therapy is preferred initially for patients requiring hospitalization:
- Treat based on local resistance for 7-14 days, longer if no source control.
- Critically Ill:
- Patients with patients with acute complicated UTI who are critically ill (ie, with severe sepsis or otherwise warranting intensive care unit admission), getting worse on current therapy, or who have suspected urinary tract obstruction (eg, if the renal function has declined below baseline or if there is a decline in urine output)
- An antipseudomonal carbapenem (imipenem 500 mg intravenously [IV] every six hours or meropenem 1 g IV every eight hours) to cover extended-spectrum beta-lactamase (ESBL)-producing organisms and Pseudomonas aeruginosa
- Vancomycin to cover methicillin-resistant Staphylococcus aureus (MRSA). Daptomycin and linezolid are alternatives to vancomycin.
- Not critically ill, hospitalized:
- Ceftriaxone 1 g IV once daily (preferred)
- Levofloxacin 750 mg IV or orally daily
- Ciprofloxacin 400 mg IV twice daily
- Ciprofloxacin 500 mg orally twice daily
- Not critically ill, hospitalized, MDR risk:
- Piperacillin-tazobactam 3.375 g IV every 6 hours or
- Cefepime 2 g IV every 12 hours (not for ESBL risk) or
- An antipseudomonal carbapenem (if recent ESBL isolate):
- Imipenem 500 mg IV every 6 hours infused over 3 hours or
- Meropenem 1 g IV every 8 hours infused over 3 hours
- Outpatients:
- For patients with low risk of fluoroquinolone resistance/toxicity:
- Ciprofloxacin 500 mg orally twice daily for 5 to 7 days or
- Ciprofloxacin extended-release 1000 mg orally once daily for 5 to 7 days or
- Levofloxacin 750 mg orally once daily for 5 to 7 days
- For patients who cannot use a fluoroquinolone:
- One dose of a long-acting parenteral agent:
- Ceftriaxone 1 g IV or IM once or
- Ertapenem 1 g IV or IM once or
- Gentamicin 5 mg/kg IV or IM once or
- Tobramycin 5 mg/kg IV or IM once
- Followed by one of the following:
- TMP-SMX one double-strength tablet orally twice daily for 7 to 10 days or
- Amoxicillin-clavulanate 875 mg orally twice daily for 7 to 10 days or
- Cefpodoxime 200 mg orally twice daily for 7 to 10 days or
- Cefadroxil 1 g orally twice daily for 7 to 10 days
- One dose of a long-acting parenteral agent:
- For patients with low risk of fluoroquinolone resistance/toxicity:
- Outpatients with MDR Risks:
- Ertapenem 1g IV or IM once
- Followed by:
- Ciprofloxacin 500 mg orally twice daily for 5 to 7 days or
- Ciprofloxacin extended-release 1000 mg orally once daily for 5 to 7 days or
- Levofloxacin 750 mg orally daily for 5 to 7 days
- UTI in Pregnancy
- You do treat asymptomatic bacteriuria in pregnancy.
- 5-7-day treatment for most (fosfomycin 1 day, Bactrim 3 days).
- amoxicillin 500 mg orally every 8 hours or 875 mg orally every 12 hours
- amoxicillin-clavulanate 500 mg orally every 8 hours or 875 mg orally every 12 hours
- cephalexin 250-500 mg every 6 hours, cefpodoxime 100 mg every 12 hours, or cefuroxime 250 mg every 12 hours
- fosfomycin 3 g as a single dose (one day)
- nitrofurantoin 100 mg every 12 hours – good for severe PCN allergy (generally avoided during the first trimester)
- Trimethoprim-sulfamethoxazole 800/160 mg (1 double-strength tablet) every 12 hours (3 days) Typically avoided during the first trimester and at term
- avoid FQs, tetracyclines, aminoglycosides, and Bactrim in last trimester due to folate antagonism
- recurrent cystitis
- longer treatment (2-6 weeks)
- If patient has 2 or fewer recurrent infections, use patient initiated therapy
- If patient has 3 or more and they are related to sex, use intercourse prophylaxis with Bactrim, cephalexin or nitrofurantoin
- If 3 or more not related to sex, daily or 3 times a week prophylaxis with
- Bactrim, cephalexin or nitrofurantoin
- Catheter-related UTI
- About 5% of patients with catheter will develop a UTI per day (by day 30, up to 95% will have UTI).
- Only treat symptomatic patients.
- Usually caused by E.coli, candida, enterococcus, Pseudomonas, K. pneumonia, Enterbacter
- Treat for 7 days if symptoms resolve promptly, 14 days if not
- Prostatitis and epididymitis
- Usually gram – organisms
- Treat for 4 weeks
- For chronic bacterial prostatitis, give therapy for 1-4 months with Bactrim or a fluoroquinolone
- Epididymitis
- If older than 35, probably caused by enteric organisms. Treat for 10 days to 4 weeks.
- If younger than 35, probably gonococcal or chlamydial. Treat with ceftriaxone 250 mg times one and doxycycline BID for 10 days.
- Gram – bacteremia due to UTI
- Most are uncomplicated BSI if source control is achieved (see Urosepsis below for more).
- Critical illness or urinary obstruction:
- For patients with patients with acute complicated UTI who are critically ill (ie, with severe sepsis or otherwise warranting intensive care unit admission), getting worse on current therapy, or who have suspected urinary tract obstruction (eg, if the renal function has declined below baseline or if there is a decline in urine output), an antipseudomonal carbapenem (imipenem 500 mg intravenously [IV] every six hours or meropenem 1 g IV every eight hours) to cover extended-spectrum beta-lactamase (ESBL)-producing organisms and Pseudomonas aeruginosa, as well as vancomycin to cover methicillin-resistant Staphylococcus aureus (MRSA). Daptomycin and linezolid are alternatives to vancomycin.
- For patients with abscesses prior to draining, as above.
ESBLs Are a Growing Risk in UTI
Risk Factors:
- Previous exposure to antibiotics (especially cephalosporins) is the largest risk
- Previous hospitalization
- UTI history/Recurrent UTIs
- Congenital urological abnormalities
- One study found swimming in freshwater was a risks.
- These are especially important in patients with urosepsis. You likely want to empirically start a carbapenem.
The DOC for ESBL in inpatients is usually a carbapenem. For outpatients with uncomplicated cystiss, you might be able to use nitrofurantoin 100 mg twice daily for 5 days, or sulfamethoxazole/trimethoprim 800mg/160mg (Bactrim DS) 1 tablet twice daily for 3 days if susceptible. For pyelonephritis or urosepsis, nitrofurantoin is not appropriate. For susceptible pathogens, Bactrim may enable early discharge as an effective oral antibiotic treatment option for UTIs caused by ESBL-positive pathogens. You can also consider Levaquin/Cipro, depending on susceptibilities.
Urosepsis:
You usually DO get a positive culture in sepsis from urinary pathogens. That’s good. You can treat according to susceptibilities.
- The most common pathogen causing urinary tract infections (UTIs), and in turn urosepsis, is Escherichia coli (50%), followed by Proteus (15%), Enterobacter (15%), Klebsiella (15%), Pseudomonas aeruginosa (5%), and gram-positive bacteria (15% – enterococci or Staph. saprophyticus )
- Urinalysis
- Urosepsis is nearly always accompanied by pyuria. Absence of pyuria largely excludes urosepsis (unless the patient is neutropenic or an obstruction is present).
- Initial fluid resuscitation with crystalloid is still recommended at a minimum of 30 mL/kg. Consider early administration of vasopressor support to maintain a mean arterial pressure greater than 65 mm Hg. The first choice for vasopressor support in sepsis is norepinephrine (with epinephrine and vasopressin 2 and 3).
- Possible Causes:
- Cystitis (usually not)
- Pyelonephritis
- Urinary obstruction (usually a stone).
- Emphysematous pyelonephritis (necrotizing pyelonephritis)
- Diverticulitis
- Acute bacterial prostatitis
- Prostatic abscess
- Renal abscess
- Urolithiasis
- It’s important to get imaging and a good diagnosis. Antibiotics alone won’t usually fix obstructions or abscesses. You need source control and/or stent placement.
- Treatment:
- You typically only need 1 antibiotic for urosepsis, but there are conflicting sources on which antibiotic you need. You will usually get a culture result, so reassess in 48-72 hours when that comes back.
- The IDSA is going to release “complicated urinary tract infection” guidelines to address this in 2025. For now:
- Zosyn: Lower rate of causing C. difficile than other broad-spectrum antibiotics, but its not great for ESBLs (can be active).
- Meropenem: Excellent coverage for AmpC enterobacteriaceae as well as ESBL gram-negatives. Can be good for hospital acquired urosepsis, or if suspected ESBL, but it has a high rate of C. difficile.
- Cefepime: No ESBL coverage, but it does cover AmpC enterobacteriaceae. Misses all enterococci species. Enterococci is intrinsically resistant to all cephalosporins.
- Ceftriaxone: Has no enterococcal coverage, no ESBL or AmpC coverage, and overuse has started to reduce the sensitivity of E. coli in many areas. In addition, it has poor urinary concentrations (it’s cleared by the liver). It’s not ideal for the sickest patients, but it’s usable if not in septic shock.
- Aminoglycosides: Nephrotoxic, hard to dose. Can be used in combination therapy.
- Fluoroquinolones – E. coli resistance to fluoroquinolones is growing and fluoroquinolones induce the emergence of multi-drug resistant bacteria more than most antibiotics. They also have a high rate of C. difficile.
- Treat for 7-14 days (lots of evidence for 7 day treatment).
- Gram + Cultures:
- If cultures are gram-negative, most of the above will work but if gram + cultures come back and the patient is deteriorating and/or on an antibiotic without enterococci coverage (like ceftriaxone or cefepime – enterococci is intrinsically resistant to cephalosporins), de-escalate to gram + coverage:
- Most patients will have Enterococcus faecalis and can be narrowed to ampicillin
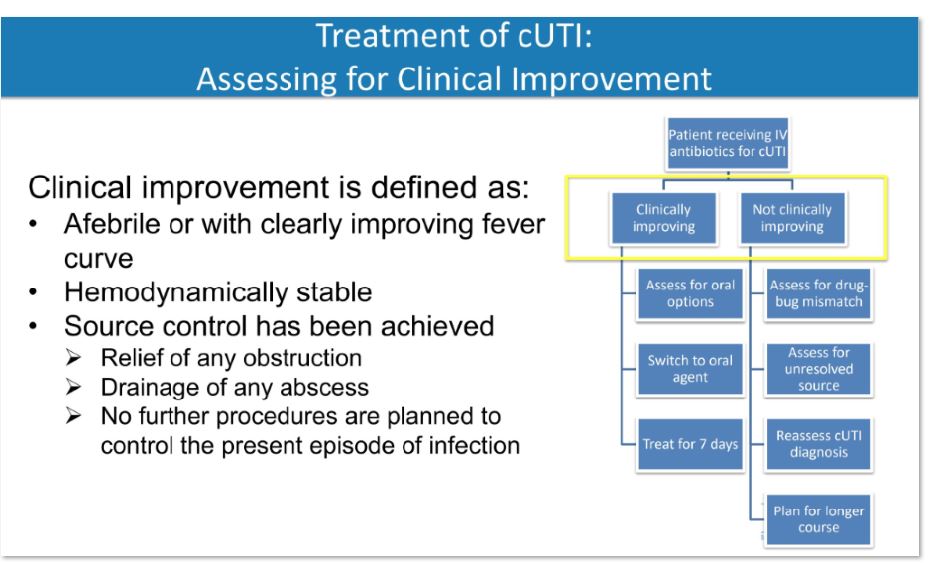
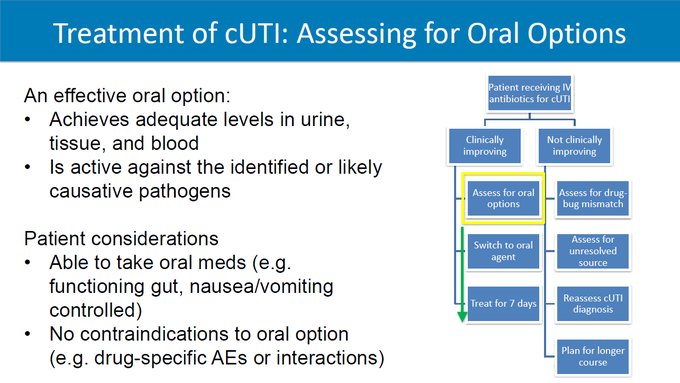
De-escalate with cultures:
- Iv to PO: Can the absorb PO (off pressors, etc).
- Can the absorb PO?
This is a preview of the upcoming guidelines: