
Molds vs Yeast 1. Antifungal Drug Classes & Mechanisms of Action A. Polyenes Examples: Amphotericin B (deoxycholate & lipid formulations), NystatinMOA: Spectrum: Key Toxicities: Role in Therapy: B. Azoles Examples: Fluconazole, Itraconazole, Voriconazole, Posaconazole, Isavuconazole, Ketoconazole, Clotrimazole, MiconazoleMOA: Spectrum: Intrinsic resistance (see above table): PK Highlights: Key Adverse Effects: C. Echinocandins Examples: Caspofungin, Micafungin, AnidulafunginMOA: […]
Antimicrobial Synergy
Synergy Synergy is often defined as when the effect of two or more agents is greater than the sum of the individual agents and often used to overcome resistance. Typically, it is suggested to give the Beta-lactam first and then give the other antibiotic fairly soon after. This has been shown to decrease mortality. Beta-lactams […]
Drug Fever
Common Causes of Drug Fever Class Drugs Antimicrobials Acyclovir, carbapenems, cephalosporins, tetracyclines, mebendazole, nitrofurantoin, penicillins, rifampin, sulfonamides, vancomycin Anticonvulsants Barbiturates, carbamazepine, phenytoin Antidepressant Doxepin, nomifensine Antineoplastic agents 6-mercaptopurine, bleomycin, chlorambucil, cisplatin, arabinoside, daunorubicin, hydroxyurea, interferon, L-asparaginase, procarbazine, streptozocin, vincristine Cardiovascular drugs Clofibrate, diltiazem, dobutamine, furosemide, heparin, hydralazine, hydrochlorothiazide, methyldopa, oxprenolol, procainamide, quinidine, triamterene Histamine-2 blockers […]
The Venomous Origins of Ozempic

In the foothills of a canyon in Arizona, a predator patiently awaits her next meal. Despite its ominous name, the Gila monster resembles more of a sluggish dragon than a true monster. It moves slowly, is active primarily in the early morning, and is not much of a hunter. Its diet consists mainly of eggs, […]
Quick and Dirty IV to Oral (PO) Choices
Some IV to PO conversions are easy (linezolid, azithromycin), but some require more thought. If a provider wants some IV to PO suggestions, the following are some to consider. These choices can be more complex than a 1:1 conversion (for example, ceftriaxone IV to PO conversion for a UTI will likely be different than for […]
Vancomycin Tips
Vancomycin 2020 Dosing Guidelines ASHP To Load or Not Load The 2020 vancomycin dosing guidelines offer these guidelines for loading doses: Why Do We Use AUC “Bayesian” Dosing? Although vancomycin historically has been classified as a concentration-dependent antibiotic. In more recent years, it has been classified as “exposure” or “AUC-dependent.” What this means is that […]
The Hitchhiker’s Guide To Antimicrobials
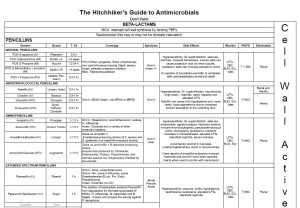
This is a resource that I used to update quite frequently and give to students, but I kind of forgot about it until a past student asked me if I still had it. I updated it this week because it was a pretty handy resource, but it was kind of out of date. You can […]
Degradation Properties of Beta-Lactamases
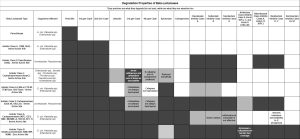
This may look better in PDF Form. I have a whole section on resistance too. *These are basics, it’s a little more complicated in some cases.Grey is degraded, lighter grey is possible.
Extended Infusions: What’s Up With That?
Extended infusions (and continuous infusions) are all the rage. Why do they work for some drugs and not others? First, we have to look at the pharmacokinetics of the drugs. Beta-lactams are the most common drugs given by extended or continuous infusion. Beta-lactams are most effective when their plasma concentrations persistently exceed the minimum inhibitory […]
Infections in Immunocompromised Patients

Typically, these regimens are tailored to these complex patients and guidelines serve as a starting point. Practitioners must consider current meds, immunosuppression, and individual patient risks. These practices also vary by site and individual practitioner. Kedia, S., Acharya, P.S., Mohammad, F., Nguyen, H., Asti, D., Mehta, S., Pant, M., & Mobarakai, N. (2013). Infectious Complications […]