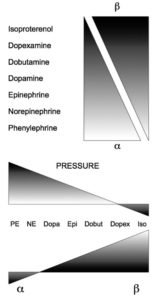
Drug Name Receptor affected HR BP CO Cardiac Vasoconstriction Peripheral Vasculature (B2) Uses Norepinephrine α, β1 ↔ ↑↑↑ ↔ or ↑ ++++ 0 2-40 ug/mincardiogenic shock Epinephrine α, β1, β2 ↑↑↑ ↑↑↑ ↑↑↑ ++++ increased peripheral vasodilation 1-20 ug/mincardiogenic shock and anaphylaxisepi activates everything) Dopamine α, β1, dopaminergic ↑↑ ↑ ↑↑ 0 increased peripheral vasodilation and […]
shock
Shock
Hypovolemic shock: Restore intravascular volume and oxygen carrying capacity. If hemoglobin < 7, administer blood products. Patients may need pressers. Obstructive shock: Must treat actual obstruction. Fluids may improve end-organ perfusion temporarily. Vasodilatory shock: Usually sepsis Septic Shock: Treat with sepsis bundles. Within 3 hours: Obtain labs. Start broad-spectrum antibiotics, ideally within the first hours (obtain […]
Hypersensitivity Reactions

Type 1 Hypersensitivity is IgE mediated. It’s anaphylaxis and the one we’re most concerned with in critical care. Treatment: Epinephrine, Benadryl, albuterol or racepinephrine, IV fluids, and pressors Steroids will help biphasic reaction, but not acute reaction. Monitor for 4-6 hours. Keep overnight if you have to re-intervene. Send home with 2 epi-pens, oral steroids for 3-5 […]