Causes:
- Bacterial infection is the most common cause of endocarditis, specifically viridans group strep, Staphylococcus aureus, HAECK group organisms (Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae), or Enterococcus.
- Endocarditis can also be caused by fungi, such as Candida.
- Some weird fastidious bacteria show up too, like Bartonella, Brucella, Coxiella burnetii (causes Q fever), Chlamydophila psittaci. Fastidious organisms are slow-growing and hard to culture. They often result in culture-negative endocarditis. We’ll see that in our treatment options for culture-negative endocarditis.
- In some cases, no cause can be found.
- Most endocarditis is community-acquired, but it can be hospital-acquired.
- Right-sided endocarditis is more common among IV drug users (IVDU). IVDU endocarditis is usually Staphylococcus.
- People with implanted devices or prosthetic heart valves have a higher rate of endocarditis than the general population.
- Valvular heart disease (including rheumatic heart disease) is a predisposing factor.
- Diabetes can be a predisposing factor.
- Urinary tract infections can be a precipitating factor.
- IDSA Endocarditis Guidelines (2015 update)
- 2023 WikiGuidelines
- 2023 ESC Guidelines
Presentation:
Endocarditis is quite a nasty infection and has systemic complications. Symptoms can be slow or sudden and include fever (the most common symptom), chills, and other signs of infection. Patient may also present with more severe symptoms and even heart failure. Presentation can depend on the organism. Staph has a typical presentation with fever, Janeway lesions, etc.Viridans group streptococci usually have a more gradual presentation (weight loss, off and on fevers) and usually found in patients with poor dental hygiene, damaged or prosthetic heart valves. Enterococcal endocarditis is usually found in the elderly or critically ill (usually with GI issues) and usually these patients don’t present with the typical fevers. HAECK endocarditis is usually associated with underlying structural heart disease, prosthetic heart valves, and periodontal disease and has an insidious onset, developing slowly over several weeks to months (can cause culture negative endocarditis because some of these organisms are fastidious and slow growers).
Since your heart pumps blood all over your body, endocarditis can also send infectious emboli to places outside of the heart. You can experience small areas of bleeding under the nails (splinter hemorrhages), red spots on the skin (Janeway lesions), painful nodes on the pads of fingers and toes (Osler nodes), small retinal hemorrhages (Roth spots), shortness of breath, swelling feet, kidney emboli, and even mental status changes when emboli go into the CNS. Cutaneous and CNS manifestations of infective endocarditis may indicate a worse prognosis. These patients should be started on empiric therapy immediately.
Duke Criteria:
The Duke Criteria are usually used to help diagnose endocarditis.
- Modified Duke Criteria:
- Major
- Blood cultures for typical microorganisms in 2 separate blood cultures
- A single positive culture for Coxiella burnetii or anti-phase-1 IgG antibody titer >- 1:800.
- Evidence of endocardial involvement
- Echocardiogram + for endocarditis.
- Minor
- Predisposition, predisposing heart condition, injection drug use
- Fever >38
- Vascular phenomena (emboli, infarcts, aneurysm, hemorrhage, Janeway lesions)
- Immunological phenomena (glomerulonephritis, osler nodules, roth spots, rheumatoid factor
- Microbiological evidence like positive culture
- Definite IE: Must have pathological criteria (vegetation, abscess, lesion) and meet 2 major criteria, 1 major and 3 minor or 5 minor.
- Possible IE: 1 major and 1 minor or 3 minor
- Rejected: Alternative diagnosis exists or resolution with antibiotic therapy <4 days, no pathological evidence with therapy =<4 days
- Clinical judgment always overrides these criteria. Some endocarditis presents slower or is culture-negative and may not meet these criteria.
- Major
- I like to think of the Major Duke Criteria being 2 points. They’re easy to remember: actual cultures, heart involvement, or vegetations. The Minor Duke Criteria are 1 point each and they are less definite: general signs and symptoms of endocarditis. If you have 4 or more points, you’re definite. If you have 3, you’re possible. The point system doesn’t work for every scenario possible, but it usually does.
- TTE should be performed in all suspected endocarditis cases. TEE is preferred, but it’s more expensive and invasive. If clinicians still suspect endocarditis upon a negative TTE, it may be worth doing a TEE in some individuals. TEE can be performed first when clinical suspicious are high.
- You need at least 3 sets of blood cultures at least 1 hour apart from different sites to confirm endocarditis.
Treatment:
- Cell wall antibiotics like B-lactams and vancomycin are less effective in endocarditis than in some other systemic infections. Why? These treatments work on actively dividing bacteria and bacteria in vegetations and biofilms don’t divide very quickly.
- Bactericidal antibiotics are needed for vegetation. Vegetations are thick and filled with fibrin and platelets. They are hard to penetrate. You sometimes need a combo to get bactericidal action. For example a B-lactam + an aminoglycoside could be used for synergy in an enterococcal infection.
- Prolonged duration of treatment needed. These are high inoculum infections. In most areas of infectious disease, less is better. In endocarditis, you can treat for 4-6 weeks or more. Some causes need lifetime prophylaxis.
- Day 1 of therapy is the first day of negative cultures unless valve surgery with positive culture or abscess on the valve, then day 1 starts after surgery.
- Administer antibiotics close together to optimize synergy.
- Cefazolin is more vulnerable to B-lactamse hydrolysis than nafcillin. Beta-lactamase type A hydrolyzes cefazolin. Nafcillin is first line.
- Because of the vegetations, MICs are super important. The MIC inside a vegetation is often higher than your MIC from culture (it takes more antibiotic to penetrate).
- HLAR (high-level aminoglycoside-resistant) endocarditis:
- Always test Enterococcus faecalis for resistance to PCN, ampicillin, vancomycin, aminoglycosides and maybe daptomycin, and linezolid
- HLAR enterococcus is not killed by B-lactams or vancomycin. You need synergy. It is relatively impermeable to aminoglycosides. Cell wall agents help gent get in. Gent peak ~3 mcg/ml, tough <1
- You can try double B-lactams therapy if gent resistance. Ampicillin and ceftriaxone (saturates different PCN binding proteins) are recommended.
- You can try streptomycin, but double b-lactam is easier.
- VRE:
- Linezolid is bacteriostatic so it’s not ideal
- Linezolid 600 mg every 12 hours for 6 weeks (beware that long term uses causes neuropathy)
- Daptomycin (10 mg/kg) can be combined with gentamicin, ampicillin, ceftaroline, rifampin, or tigecycline
- Daptomycin 10-12 mg/kg + Amp or Ceftaroline for 6 weeks
- Ceftaroline or Ampicillin can increase daptomycin surface binding against VRE.
- Linezolid is bacteriostatic so it’s not ideal
- HACEK: Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella
- High rate of B-lactamase production, should be assumed resistant to Amp
- If found in blood, assume endocarditis
- Sens to 3rd and 4th gen cephs and fluoroquinolones
- 4-6 weeks for native valve and 6 weeks for prosthetic
- Non HACEK Gram –: E.coli, pseudomonas (usually in healthcare), salmonella
- Treat with B-lactam and AG or FQ for 6 weeks
- Culture negative endocarditis (gets the kitchen sink):
- Can be the result of a patient getting antibiotics before coming to the hospital (from a PCP, for example) or from giving antibiotics before labs are drawn.
- Native:
- Acute: Cefepime and Vanc (usually S. aureus, B-hemolytic strep, anaerobic gram – bacilli)
- Subacute (lasting weeks): vanc + amp/sulfbactam (s. aureus, HACEK, enterococcus, fastidious gram -)
- Aspergillosis (fungal) cultures are usually negative. This cannot be ruled out.
- Prosthetic
- Time < 1 year: vanc + gent + rifampin + cefepime (staph, enterococcus, anaerobic gram – bacilli)
- >1 year: vanc + ceftriaxone (staph, enterococcus, VGs)
- Fungal endocarditis
- Risks: IV Drug use, CV device, immunosuppressed.
- High mortality.
- Usually, surgically replace the valve. Candida, most common, is usually + cultures, but aspergillosis is not.
- 2 phase treatment:
- Amphotericin B plus flucytosine for 6 weeks and surgery
- Lifelong Azole.
- You can use an echinocandin if candida.
| Organism | Treatment | Therapy Length in Weeks | Special Notes | |
| Strep viridans and other Strep (MIC =<0.12) | Native | Prosthetic | ||
| PCN-G | 4 | 6 | + gent has not demonstrated superior cure | |
| PCN-G + gent | 2 | 6 for PCN 2 for gent | + gent has not demonstrated superior cure | |
| ceftriaxone | 4 | 6 | + gent has not demonstrated superior cure | |
| ceftriaxone + gent | 2 | 6 | + gent has not demonstrated superior cure | |
| vancomycin | 4 | 4-6 | Last Resort Only | |
| Strep viridans and other Strep (MIC between 0.12 and 0.5) | ||||
| PCN-G + gent | 4 PCN 2 gent | 6 | Both gent and PCN for 6 weeks in prosthetic | |
| ceftriaxone | 4 | 6 | Only if susceptibility is known. Add gent for 6 weeks in prosthetic | |
| Strep viridans and other Strep (MIC => 0.5) | ||||
| ceftriaxone + gent | 4 ceftraxone 2 gent | 6 | Add gent for 6 weeks in prosthetic | |
| PCN-G + gent | 4 PCN 2 gent | 6 | Add gent for 6 weeks in prosthetic | |
| vancomycin | 4-6 | 4-6 | ||
| MSSA | ||||
| oxacillin or nafcillin | 6 | >=6 | add gent and rifampin to prosthetic valves | |
| cefazolin if allergic | 6 | >=6 | add gent and rifampin in prosthetic valves. Cefazolin may be more vulnerable to B-lactamases than nafcillin. | |
| vancomycin | 6 | 6 | only as last resort (add gent and rifampin to prosthetic valves) | |
| MRSA | **Linezolid is no good*** | |||
| vancomycin | 6 | >=6 | add gent and rifampin to prosthetic valves | |
| daptomycin in native valves only | 6 | High dose (8-10 mg) | ||
| enterococcus | ||||
| PCN-G or ampicillin + gent | 4-6 | 6 | ||
| vanc (only if unable to take B-lactam) + gent | 6 | 6 | *Some enterococcus that are resistant to gent will be sensitive to streptomycin. | |
| ampicillin + ceftriaxone | 6 | 6 | ||
| PCN Resistant Enterococcus | ||||
| vanc + gent | 6 | 6 | ||
| Multi-resistant enterococcus | ||||
| linezolid | >=6 | >=6 | ||
| daptomycin | >=6 | >=6 | ||
| HACEK Group | ||||
| ceftriaxone | 4 | 4 | ||
| ampicillin/sulfbactam | 4 | 4 | ||
| fluoroquinolones (cipro, moxi, levo) | 4 | 4 |
Oral Therapy/Outpatient IV:
In patients with endocarditis on the left side of the heart who were in stable condition, changing to oral antibiotic treatment was noninferior to continued intravenous antibiotic treatment. You may transition stable patients to oral, especially when outpatient IV would be difficult. Patient should receive IV antibiotics for at least 10 days.
POET Trial: the landmark trial for oral switch, though there are a few issues with it, other studies have confirmed outcomes. Iversen K, et al. “Partial Oral versus Intravenous Antibiotic Treatment of Endocarditis”. The New England Journal of Medicine. 2019. 380(5):415-424.
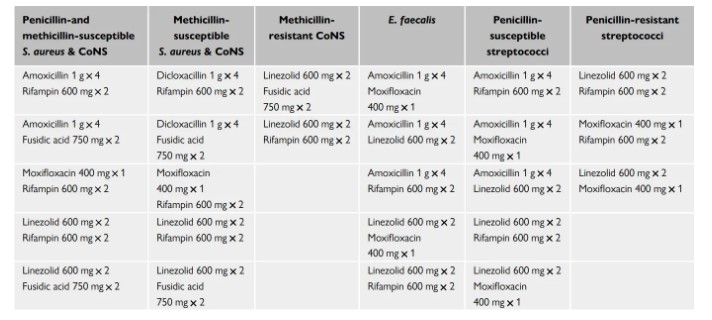
Regimens from POET:
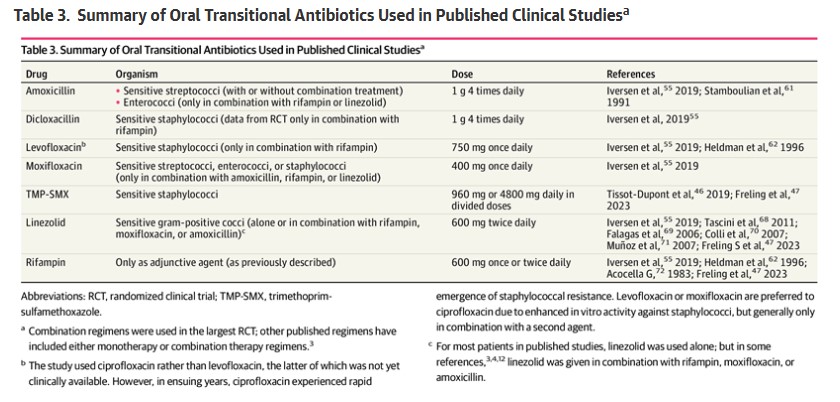
Other Oral Studies:
Take-Home Points:
- For uncomplicated, highly sensitive, native value strep endocarditis, adding gent shortens treatment to 2 weeks from 4 weeks.
- Add rifampin in prosthetic valves when the bacteria is staph. We don’t usually use it in native valves because it has potential for hepatotoxicity and drug-drug interactions, and studies have shown it actually may increase mortality risks in native valve patients.
- Staph never gets an aminoglycoside in native valves (always in prosthetics)
- Enterococcus almost always gets gent
- No daptomycin in left-side prosthetic valve endocarditis
- Patients get long courses because bacteria like to hang out in heart valve vegetations, forming biofilms of the heart that are difficult for antibiotics to penetrate Most antibiotics (like beta-lactams and vancomycin) only get actively dividing cells. Bacteria in biofilm divide slower so it takes a while to get rid of infections. Many antibiotics, such as beta-lactams and vancomycin, are most effective against rapidly multiplying bacteria. The slow division of bacteria in endocardial vegetations also allows more time for the development of antibiotic resistance. Biofilms also shield the colony, immune cells have a difficult time clearing the infection, which makes antibiotics the primary method for eradication.
Prophylaxis:
- 30% of flora in gingival crevice is viridians strep.
- High risk:
- Prosthetic heart valve or prosthetic materials used for repair
- Previous endocarditis
- Congenital heart disease: cyanotic CHD, including shunts, that is unrepaired, repaired heart defects within 6 months, repair with a prosthetic patch or device, cardiac transplant patients
- Prophylaxis is only needed for these procedures: Manipulation of gingival tissue or perforation of oral mucosa: biopsy, suture removal, placement of orthodontic bands. Also in invasive respiratory procedures: tonsillectomy, drainage of abscesses, adenoidectomy, drainage of abscesses or empyema.
- We get transient bacteria when we eat or brush our teeth. If your dental procedure isn’t worse than that, you don’t need it. Our bodies can take care of that transient bacteria.
- You only need a single dose before or up to 2 hours after the procedure
- Amoxicillin 2g PO or Amp 2g IM/IV, cefazolin, ceftriaxone
- Can use cephalexin, clindamycin, azithromycin, clarithromycin if allergic
CIED Infections:
If device is removed and blood cultures are negative, treat for 10 days. If blood cultures are positive, extended treatment will be needed. Target Staph and Pseudomonas. Can also be Enterococcus or Candida.