
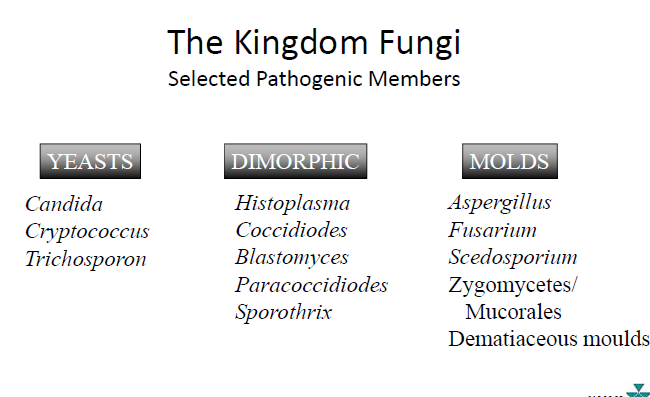
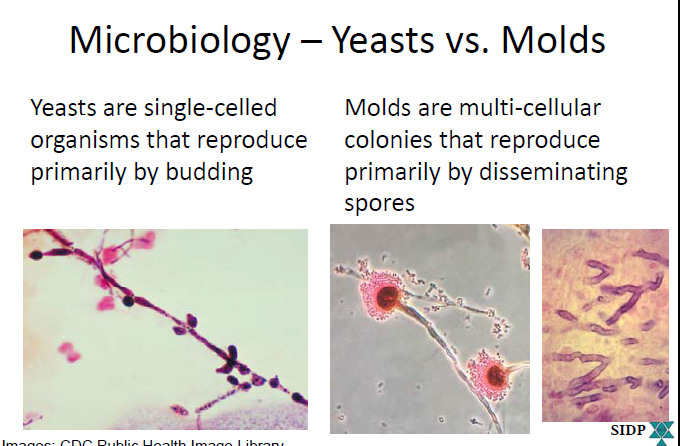
Molds vs Yeast
1. Antifungal Drug Classes & Mechanisms of Action
A. Polyenes
Examples: Amphotericin B (deoxycholate & lipid formulations), Nystatin
MOA:
- Bind ergosterol → create membrane pores → leakage → fungicidal.
Spectrum:
- Broad: Candida, Aspergillus, many molds.
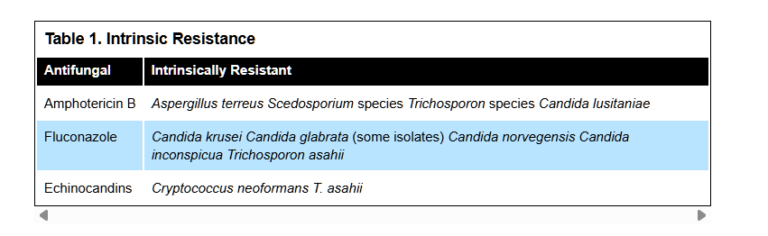
- Intrinsic resistance:
Key Toxicities:
- Nephrotoxicity (major!)
- Electrolyte wasting: ↓K⁺, ↓Mg²⁺
- Infusion reactions: fever, chills, rigors
- Lipid formulations have reduced toxicity
Role in Therapy:
- Severe or refractory invasive fungal infections
- When rapid fungicidal action needed
B. Azoles
Examples: Fluconazole, Itraconazole, Voriconazole, Posaconazole, Isavuconazole, Ketoconazole, Clotrimazole, Miconazole
MOA:
- Inhibit lanosterol 14-α-demethylase → ↓ergosterol synthesis
- Fungistatic (yeasts), fungicidal (some molds)
Spectrum:
- Variable by agent
- Fluconazole → Candida (except resistance noted below)
- Voriconazole → Aspergillus coverage
- Posaconazole/Isavuconazole → broad mold coverage
Intrinsic resistance (see above table):
- Fluconazole: Candida krusei, some C. glabrata
- Echinocandins: Cryptococcus, Trichosporon
PK Highlights:
- Good oral bioavailability (especially fluconazole)
- Hepatic metabolism (CYP450)
- Fluconazole inhibits CYP2C9
- Voriconazole inhibits CYP3A4
- Many drug interactions
Key Adverse Effects:
- Hepatotoxicity
- QT prolongation (except isavuconazole shortens QT)
- GI upset
- Voriconazole: visual disturbances, hallucinations, photosensitivity
C. Echinocandins
Examples: Caspofungin, Micafungin, Anidulafungin
MOA:
- Inhibit β-1,3-D-glucan synthesis → weakened cell wall → fungicidal vs Candida
Spectrum:
- Candida spp. (including many azole-resistant)
- Aspergillus (static)
Intrinsic resistance:
- Cryptococcus, Trichosporon (see above table)
PK Notes:
- IV only
- Minimal hepatic metabolism (anidulafungin essentially none)
- Few drug interactions
- Well tolerated
D. Miscellaneous Agents
Flucytosine (5-FC)
- MOA: Converted to 5-FU → inhibits DNA/RNA synthesis
- Spectrum: Candida, Cryptococcus
- Used with amphotericin B (cryptococcal meningitis)
- Toxicities: bone marrow suppression
Griseofulvin
- MOA: Inhibits mitosis by disrupting microtubules
- Spectrum: dermatophytes only
- Long treatment courses
2. Pharmacokinetics (PK) Overview
Absorption
- Azoles: generally good PO absorption
- Fluconazole: >90%
- Itraconazole: ~55% (needs acidic environment; food ↑ absorption)
- Voriconazole: empty stomach preferred
- Polyenes & echinocandins: poor PO absorption → IV
Distribution
- Lipophilic agents distribute widely: voriconazole, posaconazole → CNS penetration
- Protein binding:
- Fluconazole: 11–12%
- Voriconazole: 58%
- Caspofungin: 97%
Metabolism
- Azoles: CYP450 metabolism → major drug interactions
- Echinocandins: minimal metabolism
- Amphotericin B: low metabolism; slow tissue release
Excretion
- Fluconazole: renal
- Itraconazole/Voriconazole/Posaconazole: hepatic
- Echinocandins: fecal & urine (mostly unchanged)
3. Antifungal Indications & Contraindications
Indications
- Systemic infections: invasive candidiasis, aspergillosis
- Superficial infections: thrush, dermatophytes
- Prophylaxis: neutropenia, stem cell transplant, chemotherapy
Contraindications
- Azole allergy
- Severe hepatic impairment (voriconazole/posaconazole)
- Pregnancy (itraconazole, posaconazole → category C or D)
- Voriconazole: long QT syndrome
- Amphotericin B: caution in renal impairment
4. Adverse Effects & Monitoring
Azoles
- Hepatotoxicity → monitor LFTs
- GI upset
- QT prolongation
- Drug interactions (CYP inhibition)
- Increases levels of warfarin, tacrolimus, cyclosporine, etc.
Voriconazole-specific:
- Visual disturbances
- Photosensitivity → skin cancer risk long term
Amphotericin B
- Nephrotoxicity → monitor SCr, BUN, electrolytes
- Infusion reactions → pre-medicate
- Electrolyte wasting (K⁺, Mg²⁺)
- Lipid formulations decrease toxicity
Echinocandins
- Generally well tolerated
- Mild transaminitis
- Fever, infusion reactions (uncommon)
Serious Reactions (rare)
- Stevens–Johnson syndrome (azole)
- Anaphylaxis (any agent)
- Torsades (QT-prolonging azoles)
5. Prophylactic Antifungal Therapy
When to Use Prophylaxis
High-risk populations:
- Hematopoietic stem cell transplant
- AML induction chemotherapy
- Solid organ transplant
- Prolonged neutropenia
Drug Choice
- Fluconazole → Candida prevention
- Posaconazole → mold-prevention (AML, GVHD)
- Voriconazole → alternative mold-active prophylaxis
Duration
- Short-term: during neutropenia
- Long-term: chronic GVHD
Monitoring
- Look for breakthrough infections
- Biomarkers: galactomannan, beta-D-glucan
- Adjust for organ dysfunction or interactions
Challenges
- Resistance (azole-resistant Candida)
- Hepatotoxicity
- Cost
- Need for antifungal stewardship
6. High-Yield Exam Pearls
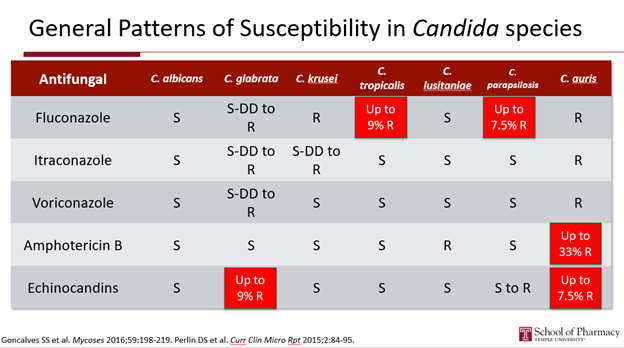
Fluconazole does NOT cover C. krusei and has poor activity vs C. glabrata.
- Voriconazole is the drug of choice for aspergillosis.
- Posaconazole is preferred for AML induction prophylaxis.
- Amphotericin B deoxycholate is much more nephrotoxic than lipid formulations.
- Echinocandins are first-line for candidemia, especially in critically ill or azole-resistant species.
- Only fluconazole has strong CSF penetration among older azoles.
- Itraconazole capsules require acid; solution does not.
- Isavuconazole shortens QT, unlike other azoles.
- Flucytosine must be combined with amphotericin B for cryptococcal meningitis
Antifungal Comparison Table
| Category | Polyenes | Azoles | Echinocandins | Misc Agents |
|---|---|---|---|---|
| Examples | Amphotericin B (all forms), Nystatin | Fluconazole, Itraconazole, Voriconazole, Posaconazole, Isavuconazole, Ketoconazole, Clotrimazole, Miconazole | Caspofungin, Micafungin, Anidulafungin | Flucytosine, Griseofulvin |
| MOA | Binds ergosterol → membrane pores → cell death | Inhibits 14-α-demethylase → ↓ ergosterol synthesis | Inhibits β-1,3-D-glucan synthase → weakens cell wall | 5-FC: inhibits DNA/RNA synthesis; Griseofulvin: disrupts mitosis |
| Fungistatic / Cidal | Fungicidal | Static vs yeasts; cidal vs molds (varies by agent) | Fungicidal vs Candida; static vs Aspergillus | Varies |
| Spectrum | Broad (Candida, Aspergillus, molds) | Wide: yeasts ± molds depending on agent | Candida (including resistant) and Aspergillus | 5-FC: Candida/crypto; Griseofulvin: dermatophytes |
| Intrinsic Resistance | A. terreus, Scedosporium, Trichosporon, C. lusitaniae | Fluconazole: C. krusei, some C. glabrata, C. norvegensis, etc. | Cryptococcus, Trichosporon | N/A |
| Key Indications | Severe invasive infections | Candidiasis, aspergillosis, prophylaxis | Candidemia, invasive candidiasis, salvage aspergillus | Crypto meningitis (5-FC); tinea (griseofulvin) |
| PK Notes | IV only (except topical nystatin); wide tissue distribution; long terminal half-life | Good oral bioavailability (flucon >90%); hepatic metabolism; many drug interactions | IV only; minimal hepatic metabolism; high protein binding | 5-FC crosses CNS; renally cleared |
| Adverse Effects | Nephrotoxicity, electrolyte wasting, infusion reactions | Hepatotoxicity, QT prolongation, GI upset; voriconazole: visual changes | Generally mild; ↑ LFTs; infusion reactions | 5-FC: bone marrow suppression |
| Drug Interactions | Minimal | Major CYP inhibitors | Few interactions | 5-FC: ↑ toxicity with amphotericin B (but used together intentionally) |
| Best Uses | Life-threatening fungal infections | Targeted use based on species + site | Critically ill pts with candidemia, azole resistance | Adjunct crypto therapy; superficial fungal infections |
| Limitations | Toxicity; IV only | Interactions; hepatic toxicity; species resistance | Only IV; no Cryptococcus | Narrow spectrum; hematologic toxicity |
8. Clinical Algorithm: How to Choose the Right Antifungal
Step 1 — Identify the Suspected / Confirmed Fungal Pathogen
A. Candida species
Check local susceptibility patterns.
- C. albicans: fluconazole OK
- C. glabrata: variable → Echinocandin preferred
- C. krusei: Fluconazole resistant → Echinocandin or Voriconazole
- C. auris: often multidrug-resistant → Echinocandin first-line
First-line treatment:
Echinocandin (caspofungin, micafungin, anidulafungin)
Step-down:
Fluconazole if susceptible & patient stable
B. Aspergillus species
First-line:
Voriconazole (best survival data)
Alternatives:
- Isavuconazole
- Posaconazole
- Amphotericin B (if azole resistant or contraindicated)
C. Mucorales (Zygomycetes – mucormycosis)
First-line:
Liposomal amphotericin B
Alternatives:
- Isavuconazole
- Posaconazole
D. Cryptococcus (esp. meningitis)
Induction:
Amphotericin B + Flucytosine
Consolidation:
Fluconazole for months
E. Dermatophytes
Griseofulvin,
OR oral terbinafine
Superficial Candida infections: topical clotrimazole/miconazole/nystatin.
F. Endemic Fungi
(Histoplasma, Blastomyces, Coccidioides)
Mild–moderate:
Itraconazole
Severe/disseminated:
Amphotericin B → step-down to itraconazole
Step 2 — Consider the Site of Infection
| Site | Best Agent(s) | Notes |
|---|---|---|
| CNS | Fluconazole, Voriconazole, Liposomal AmphoB | Fluconazole has excellent CSF penetration |
| Bloodstream (candidemia) | Echinocandin | Best mortality outcomes |
| Urinary tract | Fluconazole | Echinocandins have poor urine penetration |
| Lungs (aspergillus) | Voriconazole | Preferred unless contraindicated |
| Skin/soft tissue | Depends on organism | Dermatophytes → griseofulvin or terbinafine |
Step 3 — Assess Patient-Specific Factors
A. Hepatic Dysfunction
- Avoid or use caution: Azoles
B. Renal Dysfunction
- Avoid amphotericin deoxycholate → use liposomal formulation
- Fluconazole is renally cleared → dose adjust
C. Drug Interactions
- Avoid azoles if patient takes:
- Tacrolimus, cyclosporine, warfarin, statins, many chemo agents
- Echinocandins = lowest interaction risk
D. Severity of Illness
Critically ill / unstable patients →
Echinocandin or Amphotericin B
Step 4 — Consider Resistance Patterns
| Species | Fluconazole | Echinocandin | Notes |
|---|---|---|---|
| C. krusei | Resistant | Susceptible | Use echinocandin or voriconazole |
| C. glabrata | S-DD | Some resistance emerging | Start echinocandin |
| C. auris | Frequently R | Some R | Start echinocandin → escalate if needed |
Step 5 — Choose the Final Agent Based on All Factors
| Clinical Scenario | Best Choice |
|---|---|
| Candidemia in ICU | Echinocandin |
| Fluconazole-resistant Candida | Echinocandin |
| Aspergillosis | Voriconazole |
| Mucormycosis | Liposomal Amphotericin B |
| Cryptococcal meningitis | AmphoB + Flucytosine → Fluconazole |
| Mold prophylaxis (AML/GVHD) | Posaconazole |
| Candida prophylaxis | Fluconazole |
| UTI caused by Candida | Fluconazole (not echinocandin) |