
Asthma is pretty common. Over 25 million people in the US have it, and over 3500 people died from it in 2017. Hispanics and blacks suffer disproportionately. It’s a disease of chronic airway inflammation causing expiratory limitations including wheezing, chest tightness, shortness of breath, and cough. It can be spontaneous or triggered by exercise, allergens and irritants, or infections. Patients usually have more than one symptom. Isolated cough is usually not asthma. Exercise-related chest pain and shortness of breath need a cardiac workout.
Asthma is a disease of inflammation. COPD is a disease of obstruction. Goblet cells make mucous to get particles out of the lungs, but cilia are paralyzed and can’t move it out. The mucous obstructs the airway. That’s why we use steroids in asthma as the first line to reduce inflammation, but not in COPD.
The “Biodiversity hypothesis” states that exposure to microbes early in life provides protection against allergic and autoimmune diseases like asthma. Decreasing biodiversity is associated with increases in human immune disfunction.
Diagnosis is based on symptoms and pulmonary function tests and is most accurate before controller meds are initiated. Patients who have already been initiated should hold long-acting beta-agonists (LABA) for up to 2 days before PFTs and hold short-acting beta-agonists (SABA) for at least 6 hours. The FEV1/FVC ratio is a measurement of the amount of air you can forcefully exhale from your lungs. FEV1, or forced expiratory volume in one second, is the volume of breath exhaled with effort in that timeframe. FVC, forced vital capacity, is the full amount of air that can be exhaled with effort in a complete breath.
There are several different phenotypes of asthma: allergic asthma, non-allergic asthma, adult-onset asthma, asthma with persistent airflow limitation, and asthma with obesity.
Some guidelines break it into only two types: T-helper cell type 2 asthmas (Th2) and non-Th2. Th2 asthma is associated with poorer outcomes due to elevated immunoglobin. They also tend to have eosinophilia, elevated exhaled nitric oxide (FeNO), and more oral corticosteroid use. FeNo levels relate to eosinophils in the blood, but FeNO can be elevated for other reasons. Check for skin conditions like eczema first.
The Global Initiative for Asthma (GINA) recommends using FeNO >20 ppb as a factor when increasing ICS or considering a biologic. The American Thoracic Society (ATS) recommends using <25 ppb (20 for kids) as a determinant that eosinophilic inflammation is not likely. ICS response is less likely. A value of >50 ppb (30 for kids) means eosinophilic inflammation and ICS response are likely.
Asthma and COPD often overlap. They call this ACOS (asthma-COPD overlap syndrome). Here is a good pocket guide to the stepwise diagnose of all three syndromes.
The GINA guidelines are the most popular guidelines, but EPR-3 Guidelines are also used (I like this EPR-3 Pocket Guide).
GINA VS EPR-3
- GINA has 2 treatment goals (risk reduction and symptom control), EPR-3 has 4 (reduce impairment, reduce risk of exacerbation, controlling symptoms, and preventing asthma-related death)
- GINA has 5 treatment steps for 2 age groups (ages 5 and under and 6 and older), EPR-3 has 6 treatment steps for 3 age groups (0-4, 5-11, 12+)
- GINA has 3 levels of severity, EPR-3 has 4
- GINA favors formoterol as the long-acting beta-agonist (LABA) and requires lower doses of inhaled corticosteroids (ICS) than EPR-3.
- In 2019, GINA changed to no longer prefer LABA-only rescue. They now prefer low-dose ICS plus formoterol (a LABA)
| Levels of Control in EPR-3 | ||||
| Components | Well Controlled | Not Well Controlled | Very Poorly Controlled | |
| Frequency of Symptoms | <2 days/week | > 2 days a week, but less than daily | Multiple times daily | |
| Nighttime Awakenings | <2 times a month | 1-3 times a week | >4 times a week | |
| SABA used | <2 days a week | > 2 days a week | several times daily | |
| Interferes with Normal Activities | none | minor | extremely limited | |
| FeV1 / FVC | normal | normal or reduced <=5% | reduced >5% | |
| FeV1 % of normal | > 80% normal | 60-80% normal | < 60% of normal | |
| Exacerbation requiring steroids | 0 or 1/yer | >=2 / year | >=2 / year | |
| Recommended step of therapy | Step 1 or Maintain current step Reasses in 1-6 month Consider Step Down If controlled for 3 mo | Step 2 or Step up 1 step Reassess in 2-6 wks | Step 3 and consider oral steroids or Consider oral steroids step up 1 to 2 steps Reassess in 2 weeks | |
| Levels of Control in GINA | ||||
| Well Controlled | Partly Controlled | Uncontrolled | ||
| Daytime Asthma symptoms > 2 times per week, any nightime symptoms, reliever needed >2 times per week, any limits on activity | None in past 4 weeks | 1 or 2 in past 4 weeks | 3 or 4 in past 4 weeks | |
| Reasses in 2-3 months Can step down if well controlled | Step up one step Reassess in 2-3 months | Step up Reasses in 2-3 months unless exacerbation, then reassess in 1 week. |
The preferred rescue inhaler is no longer albuterol with GINA 2019 (I know I already said this, but it flies against everything most of us were taught, so I’ll say it over and over again). An ICS formoterol combination is the rescue. Why formoterol? It takes 3-7 minutes to take affect (similar to albuterol). It’s a LABA (long-acting beta-agonist) that has the onset of a SABA (short-acting beta-agonist). You can’t just use any LABA as a rescue. It was also the studied drug.
Previously, it was believed that PRN LABAs could cause premature patient death. The SMART trial is responsible for this original black box warning. The AUSTRI (adults) and VESTRI (kids) studies showed no increase in asthma-related deaths. LABAs upregulate corticosteroid receptors and ICSes upregulate Beta receptors. They work synergistically (and that helps decrease steroid requirements). LABAs alone may cause Beta receptor downregulation. NO LABAs ALONE FOR ASTHMA.
Step 1:
GINA (Mild Asthma):
- Low dose PRN inhaled corticosteroid (ICS) plus formoterol PRN or *Previous guidelines have not had PRN use of LABA.
- Low dose ICS when SABA is taken
- **You don’t schedule LABA until Step 3*** Controller is the same as rescue inhaler, everything is PRN.
EPR-3 (Intermittent):
- SABA as needed
Step 2:
GINA (Mild Asthma):
- Preferred rescue is ICS/formoterol still PLUS
- Low dose ICS/formoterol PRN (same as step 1) OR
- Low dose ICS alone OR
- Leukotriene modifier OR
- Low dose ICS when SABA is taken
EPR-3 (Mild Persistant):
- Low dose ICS or
- Leukotriene modifier
- Theophylline
- Cromolyn
Step 3:
GINA (Moderate Asthma)
- Low dose ICS/LABA OR
- Medium dose ICS OR
- Low dose ICS + leukotriene modifier
- Consider house dust mite sublingual immunotherapy for patients with allergic rhinitis and FEV1 >70% of expected
- Preferred rescue is ICS/formoterol still, but you can use albuterol.
- Patient shouldn’t be on two different ICS/LABA combos (ie: if you want to schedule a different LABA/ICS combo than ICS/formoterol, you would change the rescue inhaler to albuterol). You can use ICS/formoterol scheduled and PRN though.
EPR-3 (Moderate Persistant):
- Low dose ICS + LABA or
- Medium dose ICS or
- Leukotriene modifier
- Theophylline
- Zileuton
Step 4:
GINA (Severe Asthma):
- Medium dose ICS/LABA OR
- High dose ICS (add on tiotropium or leukotriene modifier) *Tiotropium is only LAMA studied in asthma (bronchodilation and dries up secretions so more useful in COPD)
- Consider house dust mite sublingual immunothearphy for patients with allergic rhinitis and FEV1 >70% of expected
- Preferred rescue is ICS/formoterol still
EPR-3 (Moderate Persistant):
- Medium dose ICS + LABA
- Leukotriene modifier
- Theophylline
- Zileuton
Step 5:
GINA (Severe Asthma)
- High dose ICS/LABA OR
- Refer for phenotypic assessment (TH2 Asthma)
- Can add add on tiotropium, anti-IgEm anti IL-5/5R, anti IL-4R
- Consider low dose oral corticosteriods
- Preferred rescue is ICS/formoterol still
EPR-3 (Severe Persistant):
- High dose ICS + LABA
- Consider omalizumab in patients with allergies
Step 6:
EPR-3 (Severe Persistant):
- High dose ICS + LABA + oral steriods AND
- Consider omalizumab in patients with allergies
Considerations when stepping up:
- Inhaler technique. Is the patient getting their dose? Most MDIs must be shaken before use, pressurized MDIs require deep and steady inhalation, patients may breathe too slow or too fast or forget to hold their breath. Some inhalers are breath activated by they still require slow and steady inhalation. Spacers sometimes help. MDIs are just as effective as updrafts and offer fewer side effects. Watch the patient use the inhaler before stepping up. Consider switching types.
- Adherence. Are they skipping doses?
- Comorbidities (see below)
- Overuse of SABA
- Mood effects
- Modifiable risk factors like smoking
Comorbities
- GERD: some asthma medications (Beta-agonists and theophylline) worsen GERD leading to cough. Patients should be treated with PPI before stepping up.
- Obesity: obese patients may have harder to control asthma due to lung strain and other comorbidities associated with obesity.
- Sinusitis: Patients with T2 asthma tend to have sinusitis frequently. Treatment with nasal corticosteroids can help.
- Pregnancy: Asthma worsens due to hormonal fluctuations during pregnancy. Budesonide is preferred in pregnancy. Pregnancy and asthma: Keeping vitamin D levels above 30 mg/mL decreases asthma risk in the fetus. Breastfeeding mothers should avoid broad-spectrum antibiotics during the first year of life.
- Exercise-Induced Asthma: Patients should warm-up for 10-15 minutes, breathe through the nose, and use a facemask to create warmth and humidity to breathe.
- Medications: NSAIDs can make asthma worse
- Infections: Viruses like influenza can worsen asthma
Acute Asthma Exacerbations:
- Steroids: no difference in oral vs IV – 80 mg of methylprednisone.
- Magnesium sulfate if not responding to steroids (IV)
- Racemic epinephrine either subQ or by nebulizer, use IV is not responding to initial albuterol.
- Antibiotics are not usually given
- Non-invasive ventilation with largest tube possible.
- Step Down – Reduce steroid dose by 50% at 3-month intervals or switch to daily dose if on low dose.
- Step Up – Increase ICS temporarily or add formoterol.
- Exercise induced asthma: B-2 agonist, LABA for prevention
- Use bronchodilator first and then ICS (open the bronchi for steroid)
Step Down
Once patient is controlled for 3 months of more, step down to see the lowest step where they remain control. You can decrease ICS dose by 25-50% every 2 to 3 months until they are back to step 1 or at the best level for the patient.
Medications:
GINA has moved away from SABAs (albuterol and levalbuterol) since SABAs do not reduce airway inflammation.
LABA:
- formoterol
- arformoterol
- indracontrol
- olodaterol
- salmeterol
ICS:
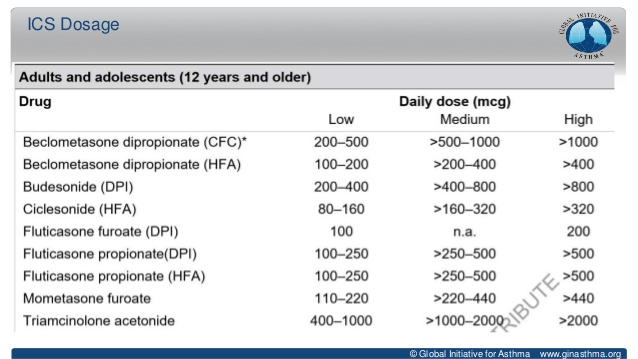
You should probably be able to tell if an ICS dose is a low dose (all < 200) or high dose (all > 400) so you can recommend therapy changes.
Oral Corticosteroids: Oral corticosteroids should be the last option. Use 7.5 mg of prednisone equivalent or less for the shortest time possible.
Anticholinergics: Evidence shows that adding tiotripium to a ICS + LABA improves lung function and reduces exacerbations
- aclindinium
- glycopyralate
- tiotropium
- umeclidium
Leukotriene Modifiers: Useful in patients who can’t tolerate higher doses of ICS (maybe kids) or have allergic rhinitis. They can also help with exercise induced asthma.
- montelukast sodium – Blackbox warning: suicidal ideations, mood changes.
- zafirlukast
- zileuton
Monoclonal Antibodies/Biologics: mostly reserved for patients with T2 Asthma, but can be used in step 4 and 5
- expensive
- Anti-IgE mAb for childhood-onset and allergen driven symptoms
- Anti-IL-5/anti-IL 5R and anti-IL-4R for T2 type asthma
- If patients don’t meet the criteria for a biologic or can’t afford one, adding tiotropium is an option.
- Most common side effects are injection site reactions, headache, and antibody development.
- Mepolizumab, benralizumab, and dupilumab can be given at home.
IgE:
- Omalizumab (XOLAIR) inhibits IgE binding to receptors on mast cells and basophils.
- Indicated in patients 6 years and older with moderate to severe asthma (can be used in child-onset).
- Need a positive skin test to an allergen (looking for a specific IgE antibody and levels) and inadequate control with ICS.
- Risk of anaphylaxis. It must be given in a health care setting. There is a slight increase in cardiovascular events associated with the drug, so screening is necessary.
- Given every 2-4 weeks.
IL5/IL5RA:
- Mepolizumab (NUCALA), reslizumab (CINQAIR), and benralizumab (FASENRA)
- These target pathways that affect eosinophils, so are indicated only in patients who have elevated eosinophil count. Patients must have had an exacerbation in the past year and eosinophil count 300 per microliter of blood or more. Better responses if eosinophil count is higher or more exacerbations.
- Better for adult-onset asthma and patients with nasal polyps present.
- Mepolizumab can reactivate herpes zoster.
- Benralizumab is only given every 8 weeks after 3 doses (others every 4 weeks)
IL4:
- Dupilumab (DUPIXENT – also for atopic dermatitis) targets a receptor for two molecules that drive allergic inflammation.
- Indicated for moderate to severe uncontrolled asthma.
- The Liberty Asthma QUEST trial foundThe most benefits was in the patients who needed maintenance oral corticosteroids.
- They need eosinophil count > 150 ul, a least one exacerbation in the past year.
- Can cause hypereosinophilia
- Given every 2 weeks