Stimulants: Try amphetamine or methylphenidate before giving up on stimulants Norepinephrine reuptake inhibitors or antidepressants if stimulants don’t work Atomoxetine, clonidine and guanfacine are also choices.***this one needs some flushing out***
Seizures: Epilepsy
*See the seizure medication table for quick reference.*Seizure Emergencies Epilepsy Treatment Options: Know doses for narrow therapeutic index drugs like phenytoin, but mostly need to know what kind of seizure and major side effects that would cause you to choose a different therapy. Also know REMS programs. Benzos can be used as adjunctive, short-term therapy (clorazepate, clonazepam, diazepam […]
Seizures: Emergent and Codes
*See the seizure medication table for quick reference. Seizure overview. Head trauma: Early seizure – within first 7 days, prevent with 5/mg/kg day phenytoin (valproate has higher mortality) No prophylaxis for late seizures. Emergent: For emergent seizures, benzos are the drug of choice to stop seizing. Lorazepam – onset 2-3 minutes, 0.1 mg/kg up to 4 […]
Seizure Medication Table
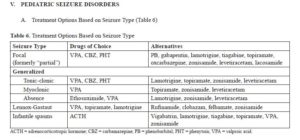
Table: 1 – first line drug, 2 – second line drug, 3 – some effect, 4 – adjunctive therapy, 5 – used only when benefits outweigh risks Drug Focal Tonic-Clonic Absence Atypical Absence Atonic Myoclonic Infantile Spasms Status Epilepticus Lennox Gastaut Acetazolamide 4 4 3 3 Brivaracetam 3 […]
Ischemic Stroke
Risk factors: Age: risks double every decade over 55 Race: more risk in native Americans, second highest risk in African Americans then whites. Sex: risk higher in men Low birth weight Family History Diabetes Hypertension Oral contraceptive use Post-menopausal hormone use Atrial fibrillation Coronary artery disease Asymptomatic carotid stenosis Dyslipidemia Obesity Physical inactivity Sickle Cell Disease […]
Parkinson’s Disease
In patients who need to be initiation on dopaminergic agents, either levodopa or dopamine agonists can be used. Levodopa is better at improving motor functions, dopamine agonists are better at lessening motor complications. May also use a MAOI (rasagiline or selegiline only, they increase extracellular dopamine). Carbidopa/Levodopa is the mainstay of therapy, but often clinicians will use […]
Headache
Acute: Treat with NSAIDS, APAP, 5-HT receptor antagonists (triptans). Prophylaxis: Avoid precipitants, TCAs, propranolol, topiramate, verapamil, valproic acid, NSAIDs, Botox, Magnesium, Vitamin B12, CoQ10, feverfew Migraine: If they are recurrent, interfere with daily activities or patient prefers prophylactic therapy, prophylaxis should be considered. Use lowest effective dose, give 2 – 3-month trial, consider a choice that also […]
Multiple Sclerosis
Acute Relapses: Methylprednisone 1g/day in divided doses for 3-5 days. Oral prednisone 1250 mg every other day for 5 days Intravenous adrenocortical hormones. DMARDs- Alemtuzumab – Can cause thyroid disorder, infusion reactions, increased infections (screen for herpes and TB before giving), may risk some cancers, vaccinate 6 weeks prior to therapy, avoid live vaccines during treatment. B – interferon […]
Schizophrenia
Diagnosis: Brief Psychiatric Rating Scale (BPRS) Positive and Negative Symptom Scale (PANSS) – 7-point, 30 item scale. Requires a 45-minute interview Positive Symptom Rating Scale (PSRS) – 1-7 scale Brief Negative Symptoms Assessment (BNSA) 1-6 scale Treatment: Antipsychotics are the first line The Joint Commission recommends 1 antipsychotic unless: 3 failed attempts at monotherapy A plan […]
Kidney Stones
There are four types of kidney stones: Calcium oxalate stones Thiazide reduces urinary calcium excretion Uric acid stones Potassium citrate – stones formed because of low urinary pH Cysteine stones – Tiopronin after dietary intervention Struvite This type of stone is found mostly in women with urinary tract infections.