
Pathogens get more complex as you move down the GI tract:
- stomach: streptococcus, lactobacilli
- pancreas (none unless necrotic)
- bile duct: E.coli, Klebsiella, Enterococcus
- small intestines E.coli, Klebsiella, Enterococcus AND diphtheroids
- distil ileum and colon: Bacteroides, Clostridium, Enterobacter, E.coli, Klebsiella, Peptostreptococcus
- Healthcare acquired adds: Candida, resistant Enterococcus, MRSA
There are lots of GI words to learn and we call GI infections weird things. These are what we call infections in the various organs.
- Appendix: appendicitis
- Gall bladder: cholecystitis
- Bile duct: cholangitis
- Pancreas: pancreatitis
- Colon: diverticulitis
IDSA Intra-abdominal Infection Guidelines
Initial treatment consists of fluid resuscitation, initiation of antibiotics, source control, and microbiologic samples. Source control is paramount if possible.
Intra-abdominal infections are classified like many other infections into community-acquired, healthcare-associated, hospital-acquired (>48 hours after hospital admission). They are also classified as uncomplicated (affects a single organ only without spread into the peritoneum) and complicated(extension beyond hollow viscus of origin into peritoneal space, peritonitis or abscess formation).
Community-acquired infections are also classified as “high risk” based on age (>70 years), immunosuppression, presence of malignancy, preexisting chronic conditions, High APACHE score (>15), healthcare-associated infections, delay in the initial intervention (>24 hours), inability to obtain source control, or exposure to healthcare.
So you have: community-acquired (complicated, uncomplicated / high risk, low risk), hospital-acquired (complicated, uncomplicated), healthcare-associated (complicated, uncomplicated /typically all high risk).
Community-Acquired Intra-abdominal Infections:
Appendicitis and diverticulitis are 2 of the most frequently diagnosed causes of complicated intra-abdominal infections. Blood/fluid cultures are not routinely needed for patients with community-acquired infection unless septic or at high-risk for MDRO infections.
Appendicitis:
Appendicitis usually needs broad-spectrum AND anaerobic coverage before surgical resection. The primary treatment option for acute appendicitis continues to be surgical, though some studies suggest antibiotics only can cure some cases. This is not recommended due to studies indicating recurrence and eventual need for removal.
| Therapy | Pediatric | Adults | |
| Mild-Moderate | High Risk | ||
| Single Agent | Carbapenems, piperacillin-tazobactam | Cefoxitin, ertapenem, moxifloxacin, tigecycline, or ticarcillin-clavulanic acid |
Carbapenems (not ertapenem) or piperacillin-tazobactam |
| Combination | 3rd- or 4th-generation cephalosporins with metronidazole OR aminoglycosides with metronidazole or clindamycin |
1st-, 2nd-, or 3rd-generation cephalosporin, ciprofloxacin, or levofloxacin, each in combination with metronidazole |
Antipseudomonal cephalosporin, ciprofloxacin, or levofloxacin each in combination with metronidazole |
*24 hours of ceftriaxone and metronidazole after surgery for a ruptured appendix
With source control, four days of therapy after surgery are usually enough (STOP-IT Trial) for complicated IAI, but 4-7 days is guideline indicated.
Diverticulitis:
Diverticulitis is Inflammation of diverticulitis in colon. Care includes bowel rest, increased fluid intake, and oral/IV antibiotic therapy for 7-14 days (usually 10 – but this is controversial) with gram – coverage, and anaerobic coverage (see above chart). Early antibiotics are important.
- CT is needed for definitive diagnosis.
- You don’t need source control in mild/moderate cases.
- Surgical resection may be needed in more severe cases. About 15% patients with acute diverticulitis develop an abscess, specifically pericolonic and intra-mesenteric. Clinically, abscess formation should be suspected if fever and leukocytosis do not subside despite adequate antibiotics. A tender abdomen and tender mass suggest possible abscess formation. Abscesses that are less than 2 cm to 3 cm can be treated conservatively with IV antibiotics. Large abscesses should be drained percutaneously with CT guidance.
- Fistula formation is another complication.
- Partial bowel obstruction or pseudo-obstruction due to colonic ileus can occur. These may also require surgical resection or prolonged antibiotic courses.
- Low-risk, uncomplicated patients may not need antibiotics.
- Antibiotic coverage: gram – and anaerobes for 10 days.
Pancreatitis
- The most important step in the management of acute pancreatitis is aggressive fluid resuscitation. Current guidelines define this as IV hydration preferably with Lactate Ringer’s(LR) at 20ml/kg bolus followed by 3ml/kg per hour.
- Oral feedings can be started immediately if the patient can tolerate them (low fat). TPN can worse pancreatitis so should be avoided whenever possible. Nasogastric feedings are preferred to nasojejunal.
- Analgesia is an important aspect of the management of pancreatitis and can include the use of intravenous (IV) opioids. Pancreatitis can be quite painful.
- Pancreatitis can also cause metabolic complications (eg, hyperglycemia and hypocalcemia) and those should be corrected.
- Antibiotics are only recommended in necrotizing pancreatitis or if extrapancreatic infection is present (e.g., cholangitis, bloodstream infection), but necrotizing pancreatitis can be hard to diagnose.
- When pancreatitis is caused by gallstones, a cholecystectomy can be performed during the same admission.
- When pancreatitis is caused by hypertriglyceridemia, standard therapy involves placing the patient on an insulin drip (this activates lipoprotein lipase) and prescribing fibrates.
- There is no role for antibiotics in acute pancreatitis in the absence of infectious complications. They are recommended if extrapancreatic infection is present (cholangitis, bloodstream infections) or if suspected or proven infectious necrotizing pancreatitis (especially to differentiate from sterile necrotizing pancreatitis).
- For necrotizing pancreatitis:
- The bacteria most frequently found in necrotizing pancreatitis are E. coli (27–35%), Enterococcus (24–26%), Staphylococcus aureus (14–16%), Staphylococcus epidermidis (15%), Klebsiella (15%) Pseudomonas sp (7–11%) and Streptococcus (4–7%)
- Carbapenems, fluoroquinolones, and metronidazole are known to penetrate the pancreas. Meropenem/Imipenem for 7-14 days or Ciprofloxacin/Levofloxacin PLUS metronidazole for 14 days (shorter duration if source control achieved: ie: Percutaneous drainage, surgical debridement, endoscopic transmural drainage)
- Some studies have reported that Zosyn (piperacillin/tazobactam) is an acceptable carbapenem-sparing option as well, though there is some controversy. The 2014 American College of Gastroenterology (ACG) Guideline and The 2020 American Gastroenterological Association (AGA) Practice Update both recommend carbapenems, or fluoroquinolones plus metronidazole. The 2019 World Society of Emergency Surgery (WSES) guidelines include piperacillin-tazobactam as the main treatment option recommendation to spare fluoroquinolones and carbapenems due to the spread of carbapenems. PK studies have shown cefepime, ceftriaxone and Zosyn have adequate penetration into necrotic regions of the pancreas. Metronidazole should be added to cefepime and ceftriaxone if used.
Cholecystitis (inflammation of the gallbladder, usually caused by stones in the bile duct):
- As bile becomes supersaturated, small crystals precipitate and become stuck in gallbladder mucus, resulting in gallbladder sludge.
- Over time, these crystals coalesce and form large stones (cholelithiasis/gall stones).
- Cholesterol stones result from increased bile cholesterol due to hepatic secretion and excess triglycerides. These will commonly eventually causes of pancreatitis.
A classic description of biliary colic includes crampy post-prandial right upper quadrant or epigastric pain radiating to the back or scapula, particularly evident following a high-fat meal, often accompanied by nausea and vomiting. If the gallbladder becomes acutely inflamed with bacterial infiltration, the pain is typically constant and progressive. Classic gallbladder pain is described as subcostal right upper quadrant pain elicited by palpation during inspiration. Pain may also present in the substernal area or left upper quadrant.
The definitive treatment for cholecystitis is surgical removal of the gallbladder. Poor surgical candidates may benefit from initial nonoperative management with antibiotics and a gallbladder drainage procedure; those whose surgical risk improves after resolution of the acute inflammation should undergo elective gallbladder surgery to prevent recurrent symptoms.
Antibiotics are indicated for all complicated acute cholecystitis cases (ie, gallbladder gangrene/necrosis, rupture, or emphysematous cholecystitis) and for uncomplicated patients who are frail, have diabetes, or are immunocompromised. Use antibiotics per above table, depending on patient presentation. Once started, antibiotic therapy should continue until either the gallbladder is removed or the cholecystitis clinically resolves. Antibiotics may be stopped the day after a clean cholecystectomy.
Acute cholangitis (a bile duct obstruction leading to infection):
- Cholangitis is a life-threatening condition caused by an ascending bacterial infection of the biliary tree. This type of infection has a high mortality rate (up to 27%)
- Initial medical therapy relies on early fluid resuscitation, electrolyte replacement, and appropriate antibiotic coverage. Delay in treatment can lead to septic shock. Depending on the course and severity, a biliary drainage procedure may be performed with the assistance of endoscopic and surgical resources
- Symptoms include fever, chills, malaise, rigors, generalized abdominal pain, jaundice, pruritus, pale stools, AST/ALT increases, jaundice. These patients usually look quite ill and can be septic.
- The first-line imaging study of choice is abdominal ultrasonography.
- Ascending cholangitis must be urgently addressed by removing the obstruction, using endoscopic instrumentation or percutaneous transhepatic intervention or surgery, and administering early antibiotics. Antibiotic treatment should be started immediately in patients with obstructive, stone-related acute cholangitis. Cholecystectomy should be performed after recovery from acute illness.
- Initiation of early intravenous antibiotics known to achieve high biliary concentrations such as fluoroquinolones, extended-spectrum penicillins, carbapenems, and aminoglycosides is required. Empirical antibiotic treatment should include molecules active on the most frequently isolated aerobic and anaerobic Gram-negative bacteria (Escherichia coli, Klebsiella, and Bacteroides). Treat for Enterococcus in hepatic disease and immunocompromised. It is recommended to start broad-spectrum intravenous antibiotics within the first hour from the onset of septic shock symptoms, and within six hours in the other cases.
- Per the Surgical Infection Society, “The potential pathogenicity of Gram-positive enterococci is not clear and targeted antibiotic therapy should not be prescribed for community-acquired infections; it should be administered, instead, for immunosuppressed or transplanted patients. Furthermore, ESBL-producing microorganisms are frequently isolated in patients with community-acquired biliary infections previously treated with antibiotics. Pharmacological administration should be chosen according to the most frequently isolated microorganisms, also considering the local trends of antibiotic resistance and drug availability. Moreover, the drug choice will depend on whether the infection is community-acquired or hospital-acquired, its severity, and the risk of the presence of MDR microorganisms. Overall, several classes of antibiotics have good biliary penetration profiles: piperacillin–tazobactam, tigecycline, amoxicillin–clavulanate, ciprofloxacin, and ampicillin–sulbactam cefotaxime and ceftazidime have good bile penetration. Antibiotics such as meropenem may have impaired pharmacokinetics due to biliary obstruction, and vancomycin and aminoglycoside, have low bile penetration.“
- The majority of patients respond to medical therapy, but some require immediate decompression. Biliary decompression or drainage can be achieved by ERCP (Endoscopic retrograde cholangiopancreatography), percutaneous transhepatic cholangiography (PTC), endoscopic ultrasonography (EUS)-guided drainage, or surgical drainage. ERCP is the gold standard and treatment of choice for biliary decompression
- Patients need 7-10 days of antibiotics if septic, 4–7 days after successful biliary drainage (with some sources suggesting 3 may be sufficient after source control). The Surgical Infection Society Guidelines recommend against the use of post-operative antibiotics in patients with mild or moderate AC.
Laparoscopic cholecystectomy is the standard of care for symptomatic gallstones. Common bile duct stones can be removed with a preoperative, postoperative, or intraoperative ERCP, or intraoperatively with a laparoscopic or open common bile duct exploration.
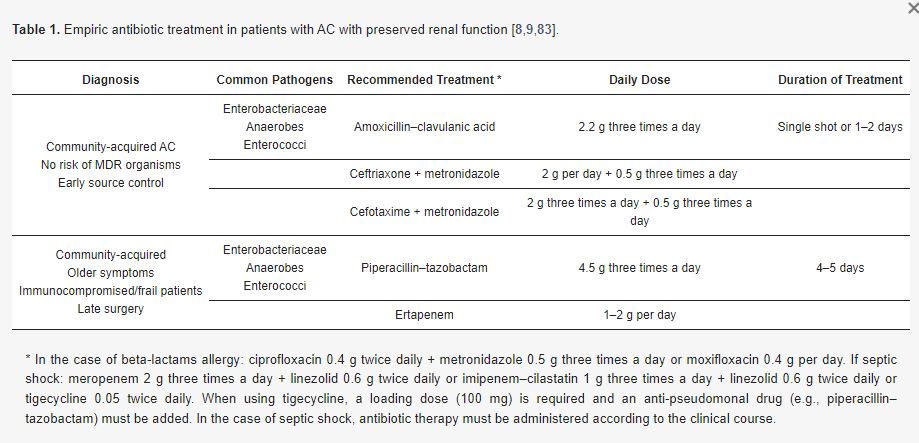
Above from the Surgical Infection Society Guidelines (AC=Acute Cholangitis)
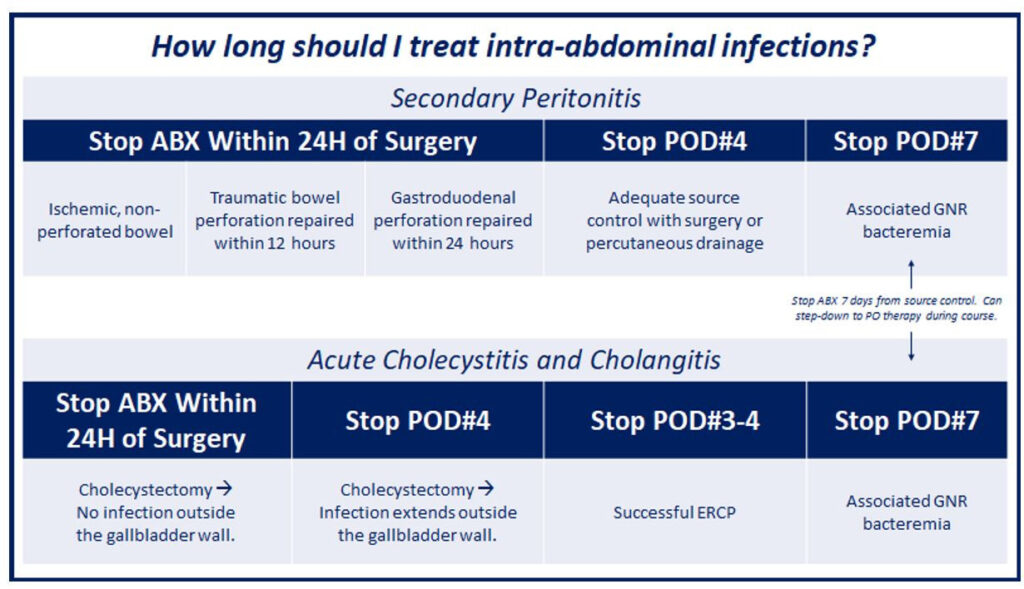
*Above graphic from the Stanford Antimicrobial Safety and Sustainability Program
Healthcare-Associated Complicated IAI
Healthcare-associated feature the presence of any of the following risk factors: invasive device at the time of admission; history of MRSA infection or colonization; history of surgery, hospitalization, dialysis, or residence in a long-term care facility in the past 12 months.
Treat according to local resistance factors or micro results. If your local antibiogram shows many ESBL-producing Enterobacterales or Pseudomonas resistance to ceftazidime or cefepime, it is recommended to add an aminoglycoside.
| Organisms seen in healthcare-associated infection at local institution |
Carbapenem | Piperacillin-tazobactam | Ceftazidime or Cefepime Each With Flagyl |
Aminoglycoside | Vancomycin |
|---|---|---|---|---|---|
| <20% resistant P. aeruginosa, ESBL producing Enterobacteriaceae, Acinetobacter, or other MDR GNB |
Yes | Yes | Yes | No | No |
| ESBL-producing Enterobacteriaceae |
Yes | Yes | No | Yes | No |
| P. aeruginosa >20% resistant to ceftazidime |
Yes | Yes | No | Yes | No |
| MRSA | No | No | No | No | Yes |
Antifungals are recommended when abdominal cultures grow candida. Usually, use fluconazole, but in patients with previous fluconazole exposure or sepsis, may consider an echinocandin.
Antimicrobial therapy is recommended when Enterococcus is grown in patients with healthcare-associated intra-abdominal infections.
Remember:
- Enterococcus are intrinsically resistant to most cephalosporins, aminoglycosides, clindamycin, and trimethoprim-sulfamethoxazole due to the expression of low-affinity penicillin-binding proteins.
- Empiric anti-enterococcal therapy is recommended for patients healthcare associate IAI patients with postoperative infection, previous use of cephalosporin (or enterococcus-selecting antibiotics as above), or valvular heart disease.
You may need MRSA coverage if previous MRSA growth or significant healthcare and antibiotic exposure.
Infectious Diarrhea
- Don’t treat “non”s: non-typhoid salmonella, non-vibrio cholera
- Campylobacter – azithromycin/cipro
- Salmonella enterica, typhi, paratyphoid – ceftriaxone/cipro
- Shigella – azithromycin, cipro, ceftriaxone
- Vibrio cholera – doxycycline (cipro if ALT)
- Yersinia enterocolitis – Bactrim
- Shiga toxic producing E.coli: leading cause of hemolytic uremic syndrome in kids (anemia, thrombocytopenia, acute kidney injury). DO NOT TREAT. Also called 0157 E.coli or STEC E.coli.
- Fecal leukocyte count and stool lactoferrin should not be used to determine who to treat
- Oral zinc can be used to reduce duration in children 6 months to 5 years in countries with zinc deficiency.
References:
- Baron TH, DiMaio CJ, Wang AY, Morgan KA. American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis. Gastroenterology. 2020 Jan;158(1):67-75.e1. doi: 10.1053/j.gastro.2019.07.064. Epub 2019 Aug 31. PMID: 31479658.
- Bonomo, R, et al, 2024 Clinical Practice Guideline Update by the Infectious Diseases Society of America on Complicated Intra-abdominal Infections: Risk Assessment, Diagnostic Imaging, and Microbiological Evaluation in Adults, Children, and Pregnant People, Clinical Infectious Diseases, 2024;, ciae346,De Campos T, Assef JC, Rasslan S. Questions about the use of antibiotics in acute pancreatitis. World J Emerg Surg. 2006 Jul 4;1:20.
- Colling K.P., Besshoff K.E., Forrester J.D., Kendrick D., Mercier P., Huston J.M. Surgical Infection Society Guidelines for Antibiotic Use in Patients Undergoing Cholecystectomy for Gallbladder Disease. Surg. Infect. 2022;23:339–350. doi: 10.1089/sur.2021.207.
- Fuks D, Cossé C, Régimbeau JM. Antibiotic therapy in acute calculous cholecystitis. J Visc Surg 2013; 150.
- Leppäniemi, A., Tolonen, M., Tarasconi, A. et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg 14, 27 (2019). https://doi.org/10.1186/s13017-019-0247-0
- Maguire C, Agrawal D, Daley MJ, Douglass E, Rose DT. Rethinking Carbapenems: A Pharmacokinetic Approach for Antimicrobial Selection in Infected Necrotizing Pancreatitis. Ann Pharmacother. 2021 Jul;55(7):902-913. doi: 10.1177/1060028020970124.
- Mazeh H, Mizrahi I, Dior U, et al. Role of antibiotic therapy in mild acute calculus cholecystitis: a prospective randomized controlled trial. World J Surg 2012; 36:1750.
- Otto W, Komorzycki K, Krawczyk M. Efficacy of antibiotic penetration into pancreatic necrosis. HPB (Oxford). 2006;8(1):43-8. doi: 10.1080/13651820500467275. PMID: 18333238; PMCID: PMC2131372.
- Pappas PG, Kauffman CA, Andes DR et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-50 DOI: 10.1093/cid/civ933
- Runyon BA, AASLD Practice Guidelines Committee. Management of adult patients with ascites due to cirrhosis: an update. Hepatology. 2009 Jun;49(6):2087-107 DOI: 10.1002/hep.22853.
- Salminen P, Paajanen H, Rautio T et al. Antibiotic therapy vs appendectomy for treatment of uncomplicated acute appendicitis: the APPAC randomized clinical trial. JAMA. 2015;313(23):2340-8 DOI: 10.1001/jama.2015.6154.
- Sawyer RG, Claridge JA, Nathens AB et al. Trial of short-course antimicrobial therapy for intraabdominal infection. N Engl J Med. 2015;372(21):1996-2005.
- Shirah GR, O’Neil PJ. Intra-abdominal infections. Surg Clin N Am. 2014;94:1319-33 DOI: 10.1016/j.suc.2014.08.005.
- Timmerhuis HC, van den Berg FF, Noorda PC, van Dijk SM, van Grinsven J, Weiland CJ, Umans DS, Mohamed YA, Curvers WL, Bouwense SA, Hadithi M. Over-and Misuse of Antibiotics and the Clinical Consequence in Necrotizing Pancreatitis: An Observational Multicenter Study. Annals of Surgery. 2023 Jan 3:10-97.
- van Rossem CC, Schreinemacher MH, van Geloven AA et al. Antibiotic duration after laparoscopic appendectomy for acute complicated appendicitis. JAMA Surg. 2016;151(4):323-9 DOI:10.1001/jamasurg.2015.4236.
- Racketa S, et al. Meropenem versus piperacillin-tazobactam for the treatment of pancreatic necrosis, Diagnostic Microbiology and Infectious Disease, Volume 109, Issue 2, 2024, 116209.
- Tenner, Scott MD, MPH, JD, FACG1; Vege, Santhi Swaroop MD, MACG2; Sheth, Sunil G. MD3; Sauer, Bryan MD, MSci, FACG4; Yang, Allison MD, MPH5; Conwell, Darwin L. MD, MSc, FACG6; Yadlapati, Rena H. MD, MHS, FACG7; Gardner, Timothy B. MD, FACG8. American College of Gastroenterology Guidelines: Management of Acute Pancreatitis. The American Journal of Gastroenterology 119(3):p 419-437, March 2024. | DOI: 10.14309/ajg.0000000000002645