Signs and Symptoms:
- Brudzinski sign and Kernig Sign
- Symptoms include fever, neck pain/stiffness, and photophobia. More non-specific symptoms include headache, dizziness, confusion, delirium, irritability, and nausea/vomiting. Signs of increased intracranial pressure have a worse prognosis.
- Can present with a rash. An erythematous macular and petechial rash in the extremities is associated with 3: Rocky Mountain Spotted Fever, syphilis, and meningococcus, but others can cause rashes too.
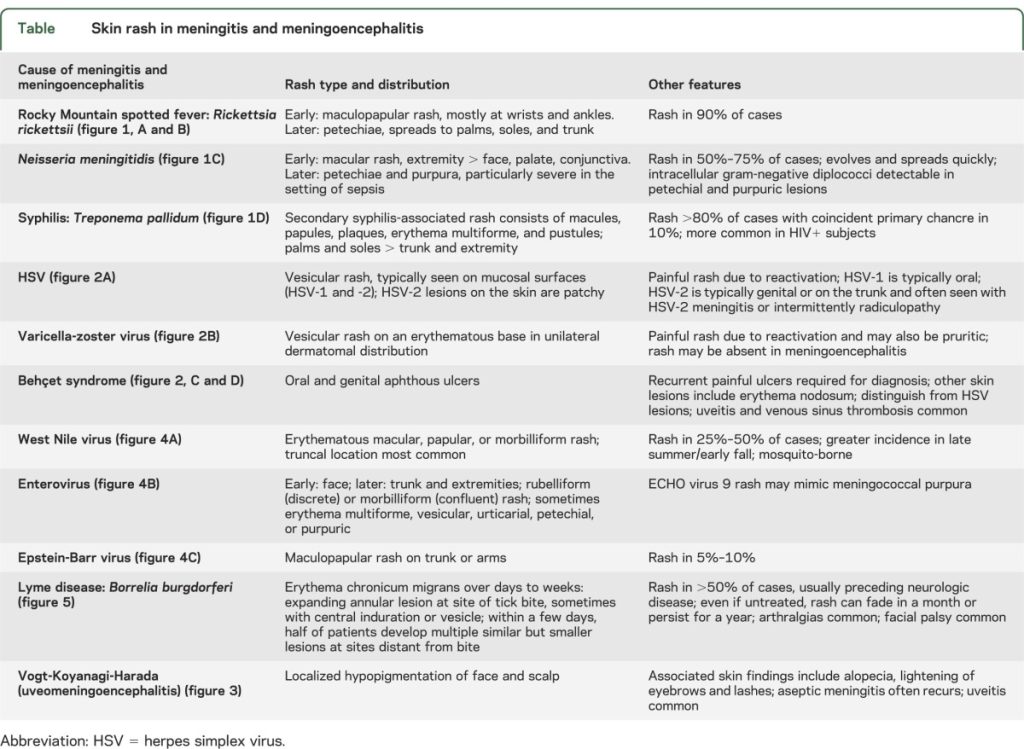
Tsai J, Nagel MA, Gilden D. Skin rash in meningitis and meningoencephalitis. Neurology. 2013 May 7;80(19):1808-11. doi: 10.1212/WNL.0b013e3182918cda. PMID: 23650233; PMCID: PMC3719428.
Treatment:
- Cover pseudomonas in penetrating trauma, post-surgical and shunts
- Dexamethasone: Some studies report a reduction in mortality for Streptococcus pneumoniae meningitis, but not in Haemophilus influenzae or Neisseria meningitidis meningitis. In children, steroids were associated with a reduction of severe hearing impairment only in cases of Haemophilus influenzae meningitis. In adults with S. pneumoniae, use of dexamethasone (versus no steroids) associated with decreased mortality. Only continue if S. pneumonia. If used, administer the first dose of dexamethasone within 10-20 minutes before or concomitant with first antimicrobial dose.
- Bactrim can replace ampicillin in penicillin allergy
- Cefotaxime is more or less equivalent to ceftriaxone, but safe in neonates (ceftriaxone may case hyperbilirubinemia, and cannot be given with calcium containing solutions)
| Age | Antimicrobial Therapy | |
| < 1 month | Ampicillin plus cefotaxime; OR ampicillin plus an aminoglycoside Streptococcus agalactiae, Escherichia coli, Listeria monocytogenes | |
| 1-23 months | Vancomycin + Ceftriaxone 100 mg/kg/day IV divided every 12 to 24 hours Streptococcus pneumoniae, Neisseria meningitidis, S. agalactiae, Haemophilus influenzae, E. coli | |
| 2-50 years | Vancomycin + Ceftriaxone 2g IV every 12h N. meningitidis, S. pneumoniae | |
| > 50 years | Vancomycin + Ceftriaxone 2g IV every 12h + Ampicillin 2g IV every 4h S. pneumoniae, N. meningitidis, Listeria monocytogenes, aerobic gram-negative bacilli | |
| Head traumas | ||
| Basilar skull fracture | Vancomycin + Ceftriaxone 2g IV every 12h S. pneumoniae, H. influenzae, group A beta-hemolytic streptococci | |
| Penetrating trauma | Vancomycin plus cefepime; OR vancomycin plus ceftazidime; OR vancomycin plus meropenem Staphylococcus aureus, coagulase-negative staphylococci (especially Staphylococcus epidermidis), aerobic gram-negative bacilli (including Pseudomonas aeruginosa) | |
| Post neurosurgery | Vancomycin plus cefepime; OR vancomycin plus ceftazidime; OR vancomycin plus meropenem Staphylococcus aureus, coagulase-negative staphylococci (especially Staphylococcus epidermidis), aerobic gram-negative bacilli (including Pseudomonas aeruginosa) | |
| Immunocompromised | Vancomycin plus ampicillin plus cefepime; OR vancomycin plus meropenem Staphylococcus aureus,S. pneumoniae, N. meningitidis, L. monocytogenes, aerobic gram-negative bacilli (including P. aeruginosa) | |
***Remember always treat for S. pneumoniae, N. meningitidis, vanc for synergy, except in newborns + a cephalosporin), listeria for the old and young (ampicillin)***
Cerebrospinal fluid makeup:
| Normal CSF | Syphilis* | Bacterial | Viral | |
| Does it Gram’s stain | No | Maybe | Yes | No |
| WBC (cells/mm3) | <5 | >20 | >1000 | <100 |
| Neutrophils | All monos | All monos | >80% | 1-50% |
| Glucose (mg/dL) | >40 | <40* | <40 | >40 |
| CSF:Serum Glucose | >0.4 | <0.4 | <0.4 | >0.4 |
| Protein (mg/dL) | <50 | >50 | >200 | >50 |
Cover pseudomonas in penetrating trauma, post-surgical and shunts: use vancomycin and cefepime 2 g IV every 8 hours or meropenem 2 g IV every 8 hours
Increased Intracranial Pressure:
If the patient develops clinical signs of increased intracranial pressure (altered mental status, neurologic deficits, non-reactive pupils, bradycardia), interventions to maintain cerebral perfusion include:
- Elevating the head of the bed to 30 degrees
- Inducing mild hyperventilation in the intubated patient
- Osmotic diuretics such as 25% mannitol or 3% saline
Prophylaxis:
If H. influenzae or N. meningitidis are cultured, household contacts and direct contacts should get prophylaxis.
N. meningitidis
- Rifampin 5-10 BID for 2 days in kids
- Rifampin 600 mg BID for 2 days in adults
- Ceftriaxone 125 mg IM times 1 < 15 years old
- Ceftriaxone 250 mg IM times 1 >15 years old
- Ciprofloxacin 20 mg/kg up to 500 mg times 1
H. influenzae
- Rifampin 20 mg/kg per dose up to 600 mg times 4 days
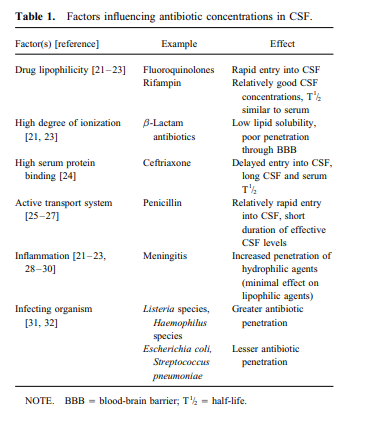
Factors affecting drug entry into the CSF: