Alcohol Withdrawal – Tremors start around 6 hours, seizures around 12 hours, but can occur 3-5 days later. Mortality can be as high as 35%. 3 Ts – Increase temp, tremor and tachycardia Treatment: correct electrolyte imbalances, benzos, can use propofol or barbiturates in refractory cases, magnesium, alpha 2 agonists, Beta blockers, calcium channel blockers Avoid: […]
Critical Care
Skeletal Muscle Relaxants
baclofen – seizure in overdose
Acid-Base Disturbances
Summary of Acid-Base Disturbances pH (7.3 – 7.4) H+ HCO3 (22-26) pCO2 (34-45) K+ metabolic acidosis ↓ ↑ ↓ ↓↓↓ ↑ metabolic alkalosis ↑ ↓ ↑ ↑↑↑ ↓ respiratory acidosis ↓ ↑ ↑↑↑ ↑ ↑ respiratory alkalosis ↑ ↓ ↓↓↓ ↓ ↓ Multiple arrows means it is a compensatory mechanism. PCo2 is usually 1.5 times the bicarb + […]
Pressors and Ionotropes
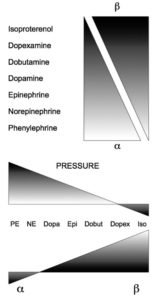
Drug Name Receptor affected HR BP CO Cardiac Vasoconstriction Peripheral Vasculature (B2) Uses Norepinephrine α, β1 ↔ ↑↑↑ ↔ or ↑ ++++ 0 2-40 ug/mincardiogenic shock Epinephrine α, β1, β2 ↑↑↑ ↑↑↑ ↑↑↑ ++++ increased peripheral vasodilation 1-20 ug/mincardiogenic shock and anaphylaxisepi activates everything) Dopamine α, β1, dopaminergic ↑↑ ↑ ↑↑ 0 increased peripheral vasodilation and […]
Shock
Hypovolemic shock: Restore intravascular volume and oxygen carrying capacity. If hemoglobin < 7, administer blood products. Patients may need pressers. Obstructive shock: Must treat actual obstruction. Fluids may improve end-organ perfusion temporarily. Vasodilatory shock: Usually sepsis Septic Shock: Treat with sepsis bundles. Within 3 hours: Obtain labs. Start broad-spectrum antibiotics, ideally within the first hours (obtain […]
Analgesics

Morphine Fentanyl Hydromorphone Onset (min) 5-10 1-2 5-10 Duration (h) 2-4 1-5 2-6 Prolonged in renal yes no no Prolonged in hepatic yes yes yes T 1/2 in hours 1-4 2-5 2-3 Active metabolites yes no no Hypotension yes no yes Flushing yes no yes Bronchospasm yes no no Constipation yes yes yes For […]
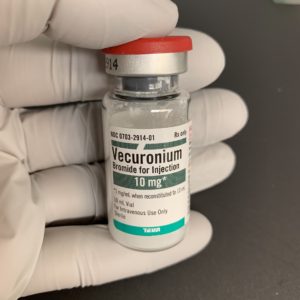
Neuromuscular Blockade and Sedation
Assessment Tools: Critical Care Pain Observation Tool (CPOT) (0-8) Behaviour Pain Scale (BPS) Sedation is Richmond Agitation Sedation Scale (RASS) or Sedation-Agitation Scale (SAS) Sedation Agents: Propofol: Rapid onset (1-2 minutes) Short duration (3-5 minutes). Avoid prolonged infusions greater than 50 mcg/kg/min. Monitor BP, triglycerides, adjust lipid calories Monitor for propofol infusion syndrome: metabolic acidosis, hemodynamic instability, cardiac […]
Hypersensitivity Reactions

Type 1 Hypersensitivity is IgE mediated. It’s anaphylaxis and the one we’re most concerned with in critical care. Treatment: Epinephrine, Benadryl, albuterol or racepinephrine, IV fluids, and pressors Steroids will help biphasic reaction, but not acute reaction. Monitor for 4-6 hours. Keep overnight if you have to re-intervene. Send home with 2 epi-pens, oral steroids for 3-5 […]