Macrocytic anemia: usually due to B12 and/or folic acid deficiency (increased MCV and MCH) Microcytic anemia: usually due to decreased iron Normocytic anemia: usually due to bleeding or chronic disease Normal MCV = 80-100 Normal MCH = 27-31
Thyroid Disorders: Hyperthyroid
Graves Disorder, pituitary adenomas, toxic goiter, drug-induced (excess thyroid hormone, amiodarone)elevated free T4, suppressed TSH Can use radioactive iodine update study to diagnose. Uptake is elevated if thyroid is excessively secreting T4 or T3: Graves disease, TSH-secreting adenoma, toxic adenoma, multinodular goiter Clinical presentation: weight loss, lid lag, heat intolerance, goiter, fine hair, tachycardia, nervousness, menstrual disturbances, sweating, […]
Thyroid Disorders: Hypothyroid
Hypothyroid Disorders: Hashimoto’s disease: Most common. Iodine deficiency most common cause worldwide. Can also be due to pituitary insufficiency or drug-induced (amiodarone, lithium). Diagnose with low free T4, elevated TSH, thyroid antibodies Symptoms: cold intolerance, dry skin, fatigue, weight gain, bradycardia, slow reflexes, coarse skin and hair, periorbital swelling, goiter, menstrual irregularities Levothyroxine is the drug of […]
Adrenal Disorders
Acromegaly – bromocriptine or octreotideHyperprolactinemia – surgical resection, cabergoline or bromocriptine Cushings Disease- Diagnosed by a dexamethasone suppression test or 24-hour urinary cortisone test. Symptoms: central obesity, peripheral fat, myopathies, osteoporosis, back pain, diabetes, hirsutism, hypertension Treatment: Surgical resection if possible Pasireotide: 0.6-0.9 mg BID subQ (adverse effects: hypoglycemia, hypocortisolism, diarrhea, nausea, gallstones, headache, bradycardia) Ketoconazole: Hinders cortisol […]
Obesity
BMI Defined: 18.5-24.9 – Normal 25.0-2939 – Overweight 30-34.9 – Class I Obesity 35-39.9 – Class II Obesity 40 or greater – Class III Obesity Treatment: Orlistat – AE: Hepattoaxity and kidney stones Lorcaserin: AE: headaches, dizziness, nausea and vomiting, dry mouth, memory or attention problems, hypoglycemia. DC if 5% weight not lost in 12 […]
Diabetes
This is a very simply rundown of diabetes. The diabetes information on the ambulatory care board exam is more complex. Knowing the basics of how to diagnose diabetes, goals, how to change insulin and which drugs not to use in which patients is probably enough for the BCPS. Pre-Diabetes Fasting Plasma Glucose: 100-125 mg/dl 2-hour […]
Ketoacidosis

Ketoacidosis is more common in type 1 diabetes than in type 2. The goal treatment is to stop ketosis, not to normalize glucose. Common symptoms: polyuria, polydipsia, vomiting, dehydration, weakness, altered mental status, coma, abdominal pain, Kussmaul respirations, tachycardia, hyponatremia, hyperkalemia Treatment: Fluid replacement: start with 0.45-0.9% NS, change to 5% dextrose or dextrose containing saline […]
Diabetes Insipidus
Decreased anti-diuretic hormone (ADH) production or lack of ADH effect.Symptoms: polydipsia, polyuria, lethargy, and confusionTreatment: desmopressin, chlorpropamide, carbamazepine for central DI, thiazide, low sodium diet and indomethacin in nephrogenic DI.
Acid-Base Disturbances
Summary of Acid-Base Disturbances pH (7.3 – 7.4) H+ HCO3 (22-26) pCO2 (34-45) K+ metabolic acidosis ↓ ↑ ↓ ↓↓↓ ↑ metabolic alkalosis ↑ ↓ ↑ ↑↑↑ ↓ respiratory acidosis ↓ ↑ ↑↑↑ ↑ ↑ respiratory alkalosis ↑ ↓ ↓↓↓ ↓ ↓ Multiple arrows means it is a compensatory mechanism. PCo2 is usually 1.5 times the bicarb + […]
Pressors and Ionotropes
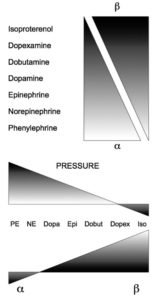
Drug Name Receptor affected HR BP CO Cardiac Vasoconstriction Peripheral Vasculature (B2) Uses Norepinephrine α, β1 ↔ ↑↑↑ ↔ or ↑ ++++ 0 2-40 ug/mincardiogenic shock Epinephrine α, β1, β2 ↑↑↑ ↑↑↑ ↑↑↑ ++++ increased peripheral vasodilation 1-20 ug/mincardiogenic shock and anaphylaxisepi activates everything) Dopamine α, β1, dopaminergic ↑↑ ↑ ↑↑ 0 increased peripheral vasodilation and […]