Low Mg, Ca or K can all cause QT prolongation
Cardiology
Acute Decompensated Heart Failure
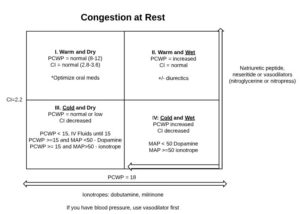
Treatment Options: Preload Reduction *Patients with diastolicdysfunction (right MI) are oftenpreload dependent, so usewith caution Loop diuretics Vasodilators Nitrogen – primarily venodilation Nitroprusside and BNP Analogs (nesiritide) are arterial and venous. Morphine ACEI, ARB, Aldosterone antagonists Afterload Reduction Vasodilators ACEI, ARB, Aldosterone antagonist Positive Inotrope Beta 1 agonist (dobutamine) Misc (high dose dopamine) Type 3 […]
Choosing Antiarrhythmics

In heart failure: only amiodarone and dofetilide Wolfe Parkinson White: procainamide or ibutilide Hypothyroid: non-DHP, avoid beta blockers Pregnancy: digoxin, non-DHP, no warfarin or heparin Do not use fenoldopam in patients with stroke, dopamine agonist can cause cerebral vasodilation and reduced blood flow to the brain 1a agents cause Torsades, usually avoid in structural heart disease 1b agents have […]
Acute Coronary Syndrome
Anticoagulant Overview: STEMI, PPCI UHF, bivalirudin STEMI, fibrinolytic UHF, enoxaparin, fondaparinux bivalirudin not studies with lytics NSTE-ACS, early invasive enoxaparin, bivalirudin, fondaparinux, UFH if you’re going to cath lab, allif placing a stent, no fondaparinux NSTE-ACS, ischemia-guided enoxaparin, fondaparinux, UFH Stop heparin after the intervention. Everyone with ACS gets dual anti-platelets for 12 […]
Congestive Heart Failure (CHF)
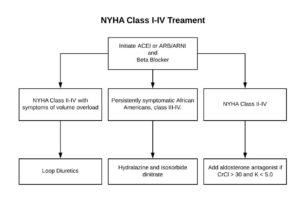
Stages of CHF: Stages of CHF NYHA Functional Class A High risk of heart failure but no structural disease or symptoms. none B Structural heart disease but without signs or symptoms of HF. I Asymptomatic HF. No limitations in physical activity caused by HF symptoms. C Structural heart disease with prior or current symptoms of […]
Atrial Fibrillation

CHA2DS2-VasC Scoring CHF or LVEF <40% Points HTN 1 Age >=75 2 Diabetes 1 Stroke, TIA, thromboembolism 2 Vascular Disease 1 Age 65-74 years 1 Sex female 1 If score is: 0 – Don’t need ASA or oral anticoagulant (OAC) 1 – ASA 2+ – OAC CHA₂DS₂-VASc Score for Atrial Fibrillation Stroke Risk (another way […]
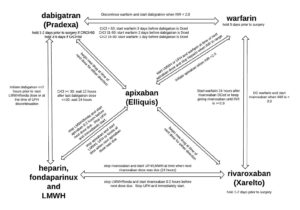
Anticoagulant Conversion Guide
Hypertensive Urgency and Emergencies (INC Aortic Dissection)

Hypertensive Urgency SBP >=180 or DBP >=110 No target organ damage Can lower over several hours or days. May not even admit. Can use oral agents like captopril, clonidine, nifedipine or labetalol. Hypertensive Emergency SBP >=180 or DBP >=110 Target organ damage (vision, neuro, kidneys, heart, etc) Avoid sudden or drastic decrease in BP Always […]
Hypertension
Blood pressure goals: Pre: < 140 and <90 (lifestyle modifications) Stage 1 HTN 140-159 or 90-99 (lifestyle and medications) Stage 2 HTN > 160 or >100 (lifestyle and 2 meds) JNC 8 When to start treatment Goal >=60 years old >=150/90 <150/90 <60 years old >=140/90 <140/90 >=18 years old + DM or CKD >=140/90 […]
Beta-Blockers
B1 Selective Blockers Non-Selective Blockers (B1 and B2) Mixed Blockers (Beta and alpha) Hydrophilic acebutolol, atenolol, bisoprolol (both), esmolol nadolol, pindolol, sotalol Lipophilic bisoprolol (both), metoprolol, nebivolol propranolol carvedilol, labetalol Some points: Avoid mixed and non-selective agents in asthma. Alpha blockade causes vasodilation, decreases peripheral resistance, and causes no reflex tachycardia. (acronym: Can Let No […]