
Stages of CHF:
| Stages of CHF | NYHA Functional Class | ||
| A | High risk of heart failure but no structural disease or symptoms. |
none | |
| B | Structural heart disease but without signs or symptoms of HF. |
I | Asymptomatic HF. No limitations in physical activity caused by HF symptoms. |
| C | Structural heart disease with prior or current symptoms of HF. |
I | |
| II | Slight limitation of physical activity. Asymptomatic at rest but symptoms with normal level of activity. |
||
| III | Marked limitation in physical activity because of HF symptoms. Asymptomatic at rest. |
||
| IV | Symptoms even at rest. Unable to carry out any physical activity. |
||
| D | Refractory HF requiring specialized interventions. |
IV | |
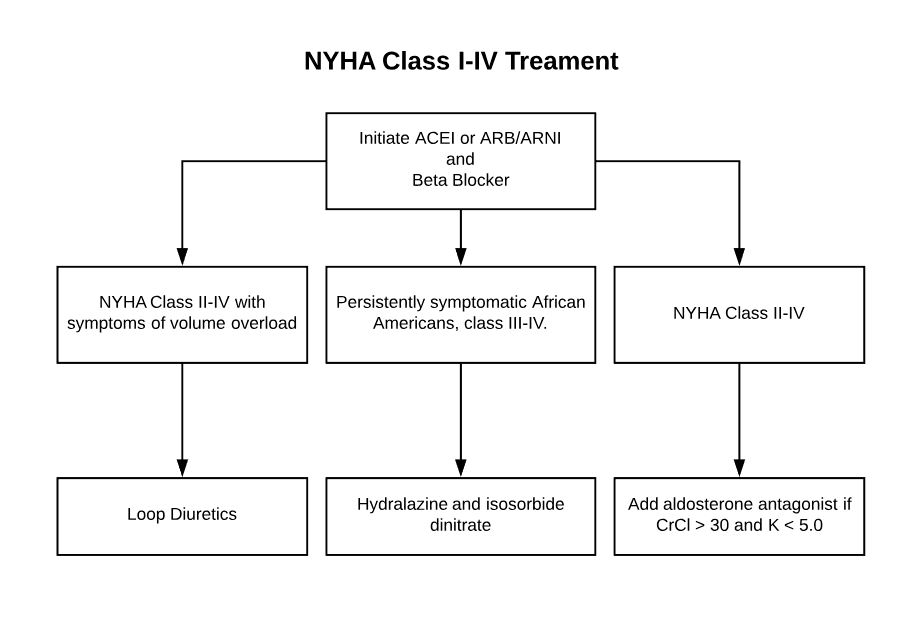
Treatments:
All patients with EF less than 40% get assessed by the five fingers of ABCDE.
- ACEI: Everyone gets ACEI or ARB. Proven to decrease mortality and symptoms. Use caution if SBP < 80, SCr > 3 or K > 5.0. Contraindicated in angioedema. Can use ARB in angioedema, but they may also cause so educate patient and use caution. Theoretically, aliskiren should not confer a risk of bradykinin-induced angioedema, because unlike ACE inhibitors, it has no known effect on bradykinin metabolism, however, caution is still recommended.
- Beta Blocker: Beta blockers decrease mortality and symptoms. The only ones used for heart failure are bisoprolol, carvedilol and metoprolol SUCCINATE only. Combine with ACEI. If hypotension is a problem, reduce ACEI before beta blocker.
- C stages of heart failure (II-IV) may get aldosterone antagonist added to ACEI and Beta blocker, especially with past cardiac hospitalization or increase in BNP or post-acute MI. Do not give if CrCl < 30.
- Digoxin can be added for symptoms. It not good at reducing exercise related dyspnea.
- Edema and fluid retention can be corrected with diuretics. There is no mortality benefit, but quality of life may improve.
- Others:
- Hydralazine/isosorbide dinitrate – add to all African Americans with III or IV stage HF>
- Sacubitril/valsartan – in stages II or III, replacing ACEI with Entresto can decrease mortality.
- Ivabradine – can reduce hospitalization in stages II and III, must be on optimal Beta blocker and have HR > 70 at rest.
- Also: be sure to control HTN, counsel on smoking cessation, EtOh abuse, correct thyroid disease and dyslipidemia.
- Calcium channel blockers with negative inotropic effects (diltiazem and verapamil) may be harmful.
Meds that Exacerbate CHF:
- Thiazolidinediones: rosiglitazone, pioglitazone
- TNF- alpha antagonist: infliximab, etanercept
- NDHP Calcium Channel Blockers: verapamil, diltiazem
- Newly Started Beta Blockers: titrate slowly
- NSAIDs/COX-2 Inhibitors: prostaglandin increases renin release, also causes fluid retention
- Glucocortocoids: sodium and water retention
- Sodium-containing medications: Zosyn, Timentin, Colace, antacids
- Itraconazole: cardiovascular toxicity
- Doxorubicin: cardiovscular toxcity
- Cilostazol: arrhythmias and death