Hypovolemic shock: Restore intravascular volume and oxygen carrying capacity. If hemoglobin < 7, administer blood products. Patients may need pressers. Obstructive shock: Must treat actual obstruction. Fluids may improve end-organ perfusion temporarily. Vasodilatory shock: Usually sepsis Septic Shock: Treat with sepsis bundles. Within 3 hours: Obtain labs. Start broad-spectrum antibiotics, ideally within the first hours (obtain […]
Analgesics

Morphine Fentanyl Hydromorphone Onset (min) 5-10 1-2 5-10 Duration (h) 2-4 1-5 2-6 Prolonged in renal yes no no Prolonged in hepatic yes yes yes T 1/2 in hours 1-4 2-5 2-3 Active metabolites yes no no Hypotension yes no yes Flushing yes no yes Bronchospasm yes no no Constipation yes yes yes For […]
Neuromuscular Blockade and Sedation
Assessment Tools: Critical Care Pain Observation Tool (CPOT) (0-8) Behaviour Pain Scale (BPS) Sedation is Richmond Agitation Sedation Scale (RASS) or Sedation-Agitation Scale (SAS) Sedation Agents: Propofol: Rapid onset (1-2 minutes) Short duration (3-5 minutes). Avoid prolonged infusions greater than 50 mcg/kg/min. Monitor BP, triglycerides, adjust lipid calories Monitor for propofol infusion syndrome: metabolic acidosis, hemodynamic instability, cardiac […]
Hypersensitivity Reactions

Type 1 Hypersensitivity is IgE mediated. It’s anaphylaxis and the one we’re most concerned with in critical care. Treatment: Epinephrine, Benadryl, albuterol or racepinephrine, IV fluids, and pressors Steroids will help biphasic reaction, but not acute reaction. Monitor for 4-6 hours. Keep overnight if you have to re-intervene. Send home with 2 epi-pens, oral steroids for 3-5 […]
Acute Decompensated Heart Failure
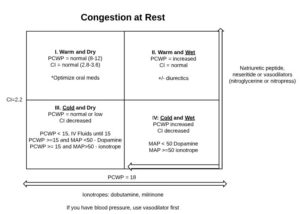
Treatment Options: Preload Reduction *Patients with diastolicdysfunction (right MI) are oftenpreload dependent, so usewith caution Loop diuretics Vasodilators Nitrogen – primarily venodilation Nitroprusside and BNP Analogs (nesiritide) are arterial and venous. Morphine ACEI, ARB, Aldosterone antagonists Afterload Reduction Vasodilators ACEI, ARB, Aldosterone antagonist Positive Inotrope Beta 1 agonist (dobutamine) Misc (high dose dopamine) Type 3 […]
Choosing Antiarrhythmics

In heart failure: only amiodarone and dofetilide Wolfe Parkinson White: procainamide or ibutilide Hypothyroid: non-DHP, avoid beta blockers Pregnancy: digoxin, non-DHP, no warfarin or heparin Do not use fenoldopam in patients with stroke, dopamine agonist can cause cerebral vasodilation and reduced blood flow to the brain 1a agents cause Torsades, usually avoid in structural heart disease 1b agents have […]
Acute Coronary Syndrome
Anticoagulant Overview: STEMI, PPCI UHF, bivalirudin STEMI, fibrinolytic UHF, enoxaparin, fondaparinux bivalirudin not studies with lytics NSTE-ACS, early invasive enoxaparin, bivalirudin, fondaparinux, UFH if you’re going to cath lab, allif placing a stent, no fondaparinux NSTE-ACS, ischemia-guided enoxaparin, fondaparinux, UFH Stop heparin after the intervention. Everyone with ACS gets dual anti-platelets for 12 […]
Congestive Heart Failure (CHF)
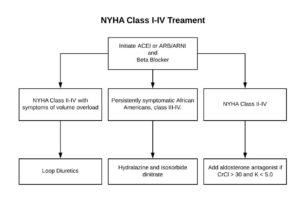
Stages of CHF: Stages of CHF NYHA Functional Class A High risk of heart failure but no structural disease or symptoms. none B Structural heart disease but without signs or symptoms of HF. I Asymptomatic HF. No limitations in physical activity caused by HF symptoms. C Structural heart disease with prior or current symptoms of […]
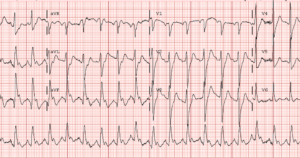
Atrial Fibrillation

CHA2DS2-VasC Scoring CHF or LVEF <40% Points HTN 1 Age >=75 2 Diabetes 1 Stroke, TIA, thromboembolism 2 Vascular Disease 1 Age 65-74 years 1 Sex female 1 If score is: 0 – Don’t need ASA or oral anticoagulant (OAC) 1 – ASA 2+ – OAC CHA₂DS₂-VASc Score for Atrial Fibrillation Stroke Risk (another way […]